
Anti-Thrombotic Fluoropolymer Promotes Safety
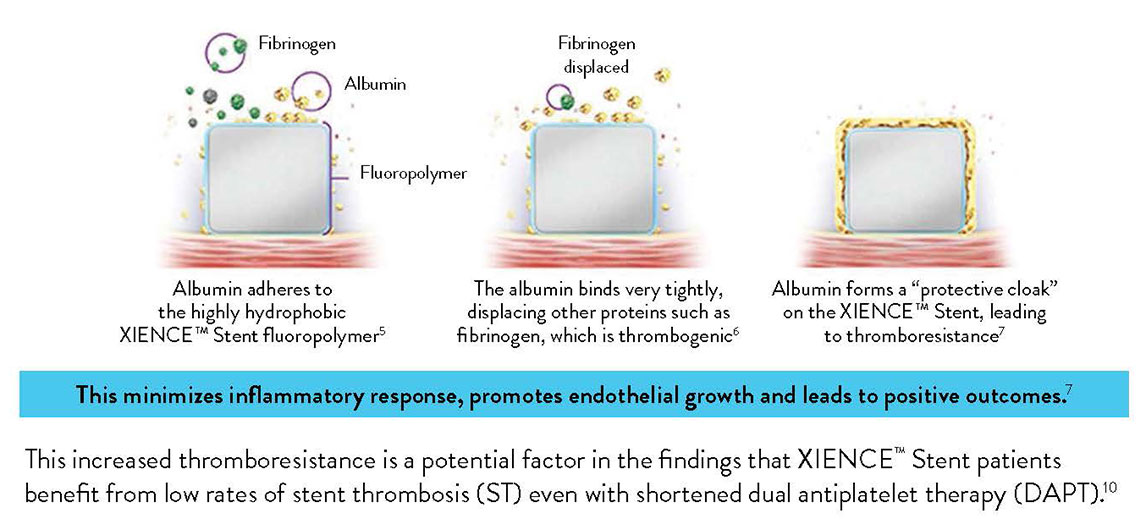
The XIENCE™ Stent polymer with a fluorinated surface has shown protective attributes—the ability to tightly bind albumin to create a “protective cloak” around the stent.2
The XIENCE™ Stent Fluoropolymer—Proven to Protect2,3
Another factor that sets XIENCE™ Stent apart is its fluoropolymer coating. Unlike other polymer coatings, the fluoropolymer interacts with proteins in the blood in a way that reduces thrombus formation—a process known as fluoropassivation.
Fluoropassivation Leads to Thromboresistance3
XIENCE™ Stent, widely considered to be the gold standard for patient safety and efficacy, is coated with a fluoropolymer.
THE XIENCE™ STENT FLUOROPOLYMER: PROVEN TO PROTECT
Due to thromboresistance and low inflammatory responses, fluorinated surfaces encourage faster endothelization and healing.4
Fluoropolymer Stent vs Bare Metal Stent and Biodegradable Polymer Stent
Moreover, the XIENCE™ Stent fluoropolymer has minimal coating defects compared to biodegradable polymer DES (BP-DES).9
In contrast to the visual above, most stents available today—biodegradable polymer stents, durable polymer stents or bare metal stents—have non-fluorinated surfaces that interact with proteins in the following ways:
- The surfaces attract less albumin and more fibrinogen.10
- The fibrinogen, in turn, leads to more platelet adhesion and activation.11
- The platelets, fibrinogen and red blood cells can aggregate and create a thrombus.12
XIENCE™ Stent Fluoropolymer vs Other Types of Stents
XIENCE™ Stent’s fluoropolymer demonstrates the fewest platelets adhering to the stent surface—an important factor in stent thrombosis.3 This fluoropolymer can protect patients from both acute and long-term complications.3,13
Representative confocal photomicrographs stained for platelets (CD42b/CD61). N=5 per stent. This preclinical ex vivo porcine shunt model used aspirin-only antiplatelet therapy.
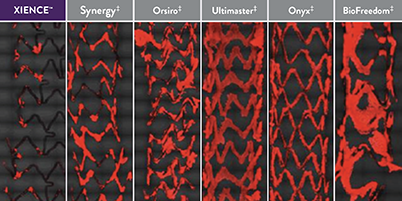
XIENCE™ Stent: Least Blood Platelet Adhesion (p < 0.01)
When Using Aspirin Monotherapy3
When Using Aspirin Monotherapy3
XIENCE™ Stent: Least Blood Platelet Adhesion (p < 0.05) When Using P2Y12 Inhibitor Monotherapy3
Representative confocal photomicrographs stained for platelets (CD42b/CD61). N=8 per stent. This preclinical ex vivo porcine shunt model used clopidogrel-only antiplatelet therapy.
XIENCE™ Stent: Least Blood Platelet Adhesion When Using Heparin Only14
Expert's Point of View: Reduced Inflammatory Response
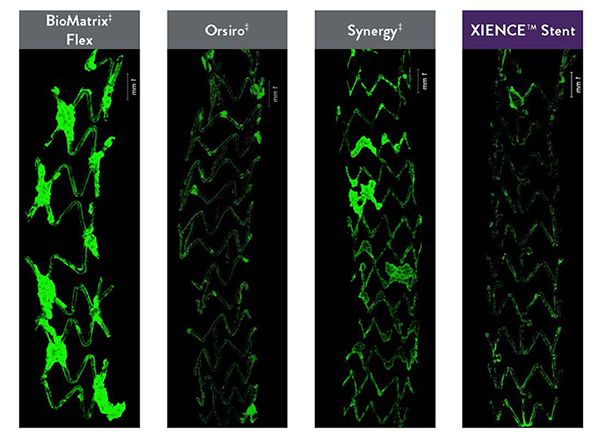
In the images “on the right you can see the [pro-thrombotic] platelet adherence. XIENCE™ Stent [the image at the bottom] has hardly any attachments to it.” — Renu Virmani, MD, referring to the photomicrographs, where green indicates platelet adhesion.
Visual Evidence of Fluoropolymer Safety
In several analyses, XIENCE™ Stent exhibits the most thromboresistance when compared to several different BP-DES.3,14
Least Thrombus Area with XIENCE™ Stent vs BP-DES14
Ex vivo porcine photomicrographs reveal the least thrombus area on XIENCE™ Stent (green areas are platelets).
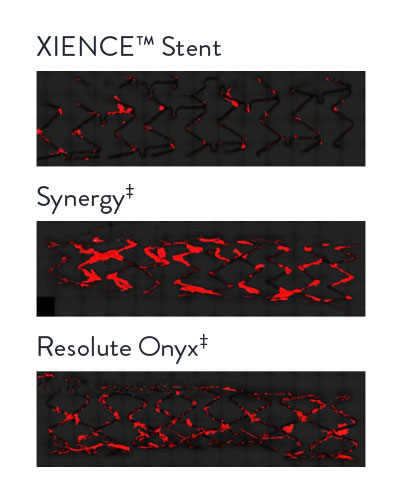
Real-Time Platelet-Device Interaction
CVPath Institute also conducted tests to show real-time platelet-device interaction between different types of stents.
XIENCE™ Stent
Compared with Synergy‡
Compared with Synergy‡
XIENCE™ Stent
Compared with Other DES
Compared with Other DES
This preclinical model used in vitro human blood with heparin only. Representative confocal photomicrographs stained for platelets. Real-time platelet-device interaction was visualized under confocal microscopy and recorded in a time-lapse video. Image processing quantified platelet deposition on devices.
References
- Zanchin C, et al. JACC Cardiovasc Interv. 2019;12(17):1665-1675. Serruys P, et al. N Engl J Med. 2010;363:136-146. Shiomi H, et al. JACC Cardiovasc Interv. 2019;12:637-647. Kufner S, et al. Circulation. 2019:139(3):325-333. Palmerini T, et al. Lancet. 2013;379:1393-1402. Bangalore S, et al. Circulation. 2012;125:2873-2891. Bangalore S, et al. Circ Cardiovasc Interv. 2013;6(6):378-390. Pilgrim T, et al. Lancet. 2014;384:2111-2122. Pilgrim T, et al. Lancet. 2018;392:737-746. Data on file at Abbott.
- Garfinkle AM, et al. Trans Am Soc Artif Intern Organs. 1984;30:432-439. Ao PY, et al. Eur J Vasc Endovasc Surg. 2000;20:241-249. Jinnouchi H, et al. EuroIntervention. 2020;EIJ-D-19-00938.
- Jinnouchi H, et al. J Am Coll Cardiol. 2019;74:(Suppl B):TCT-291. Sato Y, et al. PCR eCourse 2020.
- Szott LM, et al. Biointerphases. 2016;11:029806. Wertz CF, et al. Langmuir. 2001;17:3006-3016. Joner M, et al. J Am Coll Cardiol. 2008 Jul, 52 (5) 333-342.
- Panchalingam V, et al. ASAIO J. 1993;39:M305-M309.
- Paton DM, et al. U.S. Patent 5,356,668. Garfinkle AM, et al. Trans Am Soc Artif Intern Organs. 1984;30:43-439.
- Szott LM, et al. Biointerphases. 2016;11:029806.
- Mehran R, et al. TCT Connect 2020, XIENCE 28/90.
- Data on file at Abbott.
- Panchalingam V, et al. ASAIO J. 1993;39:M305-M309. Jinnouchi H, et al. EuroIntervention. 2020;EIJ-D-19-00938.
- Wu Y, et al. J Biomed Mater Res. 2005;74(4):722-738. Tsai WB, et al. J Biomed Mater Res. 1999:44:130-139.
- Garfinkle AM, et al. Trans Am Soc Artif Intern Organs. 1984;30:432-439.
- Kamberi M, et al. J Biomed Mater Res B Appl Biomater. 2018;106(5):1721-1729. Zanchin, C. et al. JACC Cardiovasc Interv. 2019;12(17):1665-1675. Serruys P, et al. N Engl J Med. 2010;363:136-146. Shiomi H, et al. JACC Cardiovasc Interv. 2019;12(7):637-647. Kufner S, et al. Circulation. 2019:139(3):325-333.
- Otsuka F, et al. JACC Cardiovasc Interv. 2015;8:1248-1260.
MAT-2101781 v2.0