
Experience the OCT difference.
Request your Abbott Sales rep today.
What is Optical Coherence Tomography (OCT) Imaging?
Optical Coherence Tomography (OCT) is an intravascular imaging modality that uses near-infrared light to provide high-definition, cross-sectional and three-dimensional images of the vessel microstructure during percutaneous coronary intervention (PCI).
"These images provide additional information on the degree and characteristics of coronary artery disease compared to angiography which doesn’t delineate the composition of the coronary artery.1 With automated, highly accurate measurements, OCT can guide stent selection, placement, and deployment.1"
— Dr. Manuel M. Reyes, Interventional Cardiologist
OCT Software User Interface
Ultreon™ Software is powered by artificial intelligence (AI) and automation. It has an improved and intuitive user-interface over the previous generation.*

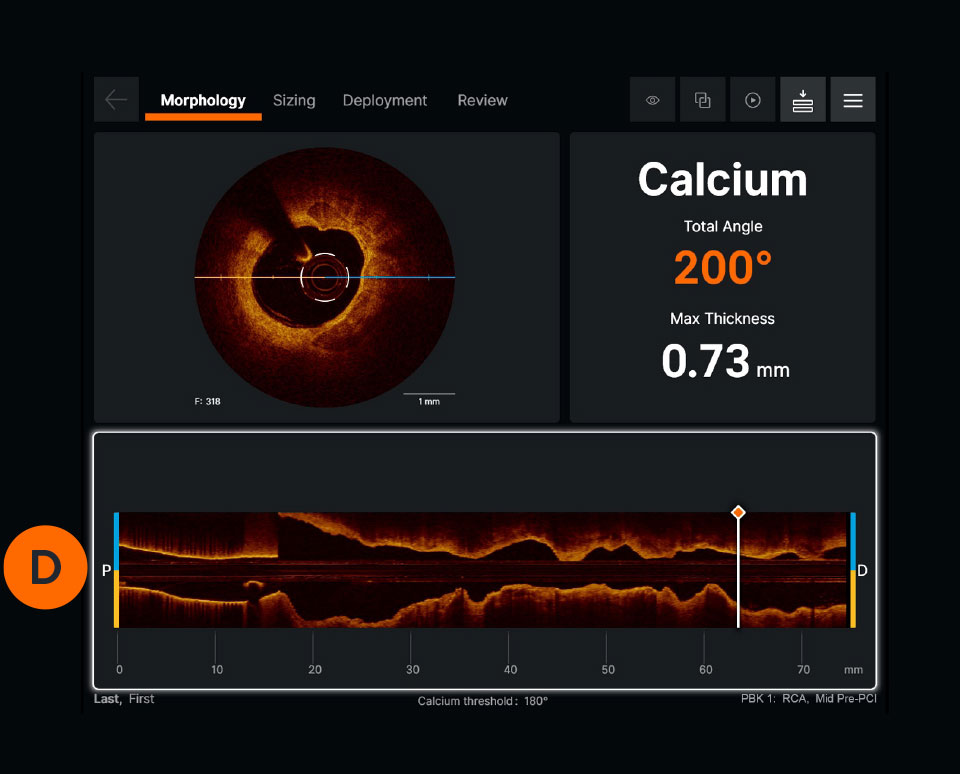
Ultreon™ 1.0 Software User Interface. Pre-PCI pullback. Automatically displays degree and max arc of calcification.
Ultreon™ 1.0 Software User Interface. Pre-PCI pullback. Automatically displays degree and max arc of calcification.
Ultreon™ 1.0 Software User Interface. Pre-PCI pullback. Automatically displays degree and max arc of calcification.
Ultreon™ 1.0 Software User Interface. Pre-PCI pullback. Automatically displays degree and max arc of calcification.
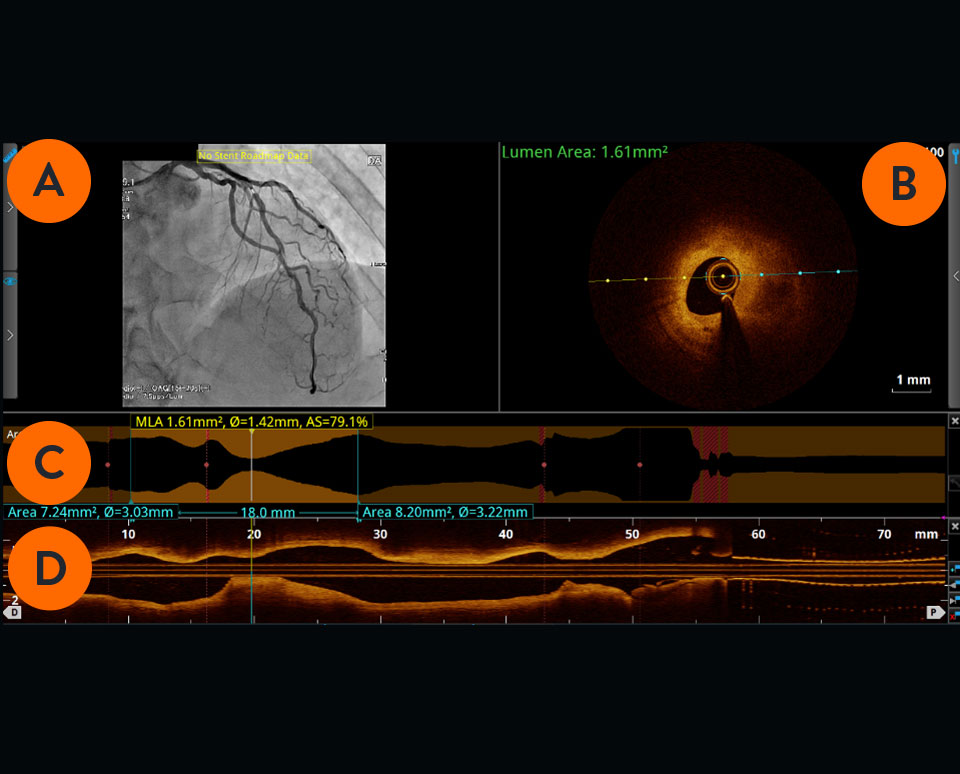
Previous generation AptiVue™ Software User Interface. Pre-PCI pullback.
Previous generation AptiVue™ Software User Interface. Pre-PCI pullback.
Angiogram co-registration denotes location of the cross-sectional OCT image.

Cross-sectional visualization is used to obtain detailed findings, such as structures in the lumen and in the various layers of the vessel wall.

The cross-sectional area of the vessel is visualized along the entire length of the examined vessel segment. It allows precise determination of the vessel diameter (mean reference diameter) and the length of the altered segment. The white marker is located at the position of the cross-section shown.

Viewed from left to right, the longitudinal section visualizes the scanned vessel segment from proximal to distal in Ultreon™ Software, and from distal to proximal in AptiVue™ Software.

How does OCT support PCI guidance?
- For pre-PCI guidance, OCT can be used to identify the culprit lesion, assess lesion morphology to select the right lesion preparation strategy, and characterize the stent landing zones to select precise length and diameter of balloons and stents.2
- For post-PCI guidance, OCT offers improved visualization of stent dissection, tissue protrusion and incomplete vessel wall apposition compared to angiography alone, thus helping to minimize stent thrombosis.3 OCT helps to confirm that stent is fully expanded to reduce stent failure.1
PCI guidance with OCT is easier now with the development of the standardized step-by-step workflow (also referred to as algorithm), MLD MAX, which is mnemonic for Morphology, Length, Diameter, Medial Dissection, Apposition and Xpansion. Using OCT with MLD MAX workflow can improve stent expansion4 without additional contrast while reducing radiation exposure compared to angiography-guided PCI.5 Stent expansion is linked to better PCI outcomes.6
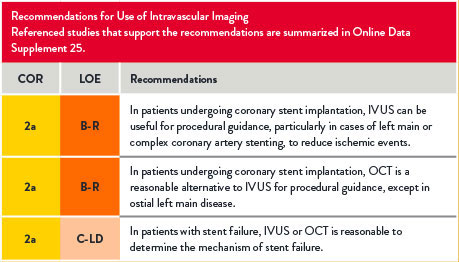
Use of Intravascular Imaging
For references, refer to the original document.
For references, refer to the original document.
Use of Intravascular Imaging
For references, refer to the original document.
The Basics of OCT
What are the OCT components?
OCT imaging systems consist of three main components: the software, the system, and the catheter.
OCT Software
Ultreon™ Software includes auto detection of certain components of the vessel based on artificial intelligence. The software is intended to be used only with compatible OPTIS™ Next Imaging Systems.
OPTIS™ Next Imaging Systems
The hardware that runs the OCT software. OPTIS™ Systems use optical imaging catheters that emit near-infrared light to produce high-resolution real-time images. The OPTIS™ Next Imaging Systems can be integrated with the cath lab angio systems to display OCT and angio co-registration (ACR) on the same screen.

OCT Catheter
The OCT catheter is intended for the imaging of coronary arteries.

OCT Image Acquisition and Interpretation
To perform an OCT pullback, an OCT catheter is inserted into the vessel and an infrared laser is used to scan the vessel wall in a spiral-like manner. The laser beam penetrates the tissue 2-3mm deep, is reflected from there and returned to the OCT device via the catheter for evaluation.7
How to set up the system for OCT-guided PCI
Watch this video to learn how to set up the OCT system. These step-by-step instructions are available on the OCT screen for easy guidance.
There are four steps to an OCT-guided PCI set up:
- Connecting syringe
- Purging the catheter
- Draping the DOC
- Connecting the catheter
How to initiate a pullback
Watch this video to learn how to initiate a pullback. The step-by-step instructions are also available on the OCT screen.
Due to the OCT systems’ high acquisition speed, images of pullback can be produced and visualized in a matter of seconds. The system provides precise information about the scanned vessel segment.7
How to interpret OCT images
Learn how to interpret OCT images, the basic elements of an OCT image and an algorithm for image interpretation.
OCT and MLD MAX Workflow
Using OCT with MLD MAX workflow, the standardized step-by-step workflow, helps to guide pre- and post-PCI decisions. Use of the workflow resulted in an 88% change in treatment decisions8 compared to angiography alone without a change in contrast usage and a 10% reduction in radiation5, as shown in the LightLab Clinical Initiative.
Six letters represent six steps of the PCI goal to MAX-imize stent expansion to deliver optimal results.
- The first three steps, MLD (Morphology, Length, Diameter) performed before PCI, designed to help inform treatment strategy.
- The last three steps, MAX (Medial Dissection, Apposition, Xpansion), performed post-PCI, to optimize stent placement. MLD MAX was developed as a part of the LightLab Clinical Initiative.
Achieving optimal expansion is proven to reduce rates of major adverse cardiac events during PCI9. Proper expansion confirmed by imaging results in safety and efficacy benefits.6
MLD-MAX-Illustration-NoIcons
Morphology
Search for High Calcium1
Criteria:
>180 degrees, and
>0.5 mm thickness, and
>5 mm in length
Length
Select Landing Zones Based on Healthy Tissue/ EEL Visualization2
Place landing zones in healthy tissue (i.e. EEL visualization)
Note: In the absence of EEL to represent healthy tissue find the largest lumen to avoid areas of TCFA or lipid pools so as to not land your stent edge in these high-risk areas3
Diameter
Measure Vessel,
Stent, Balloon Diameters4
Use distal reference measurements to select stent diameter
Use distal reference measurement for distal balloons or proximal reference measurements for proximal balloons
MLD-MAX-Illustration-NoIcons
Medial
Dissection
Address Significant Dissection2
Criteria:
Dissection penetrates medial layer, and is greater than 1 quadrant arc
Apposition
Address Gross Malapposition
Criteria:
Malapposition indicator shows longer than 3 mm4 of significant (≥0.3 mm from wall5) apposition
Xpansion
Confirm
Expansion3,6
Criteria:
≥80% acceptable,
≥90% expansion is optimal
“When we use the OCT workflow (MLD MAX), we make better decisions initially by analyzing the plaque morphology and determining appropriate vessel prep as well as selecting the appropriate stent length and diameter. By doing this, we are less likely to have to do post-PCI optimization because we are doing it right the first time. This often leads to improved procedural efficiency.”
— DR. JASON WOLLMUTH, INTERVENTIONAL CARDIOLOGIST

How to Apply MLD MAX Workflow to OCT-Guided PCI?
Watch these videos to learn more about each step of the MLD MAX workflow: Morphology, Length, Diameter, Medial dissection, Apposition, and Xpansion.
Pre-PCI Guidance: MLD | Morphology, Length, Diameter are used to determine PCI strategy.
Morphology
What is the value of morphology-guided lesion prep?
- Understanding vessel morphology and plaque characteristics (lipidic, fibrotic or calcific) allows user to determine vessel preparation strategy (i.e. if direct stenting is okay or if plaque modification is required).
- In this video, Dr. Ziad Ali provides a detailed overview of the structure of the normal vessel morphology, how it displays on OCT and shares an easy-to-use OCT image interpretation algorithm.
- Dr. Ziad Ali discusses vessel preparation strategies based on plaque type, and the influence on coronary calcium on stent expansion. Learn more about OCT in calcified lesions.
Length
Why does proper stent length matter?
Diameter
Why does accurate diameter matter?
- Appropriate sizing of stent diameter is important to limit underexpansion, malapposition and dissections.
- Angiography both over- and underestimates stent diameter to a similar degree and led to an inaccurate stent diameter in 38% of stented lesions as demonstrated in the LightLab Clinical Initiative.8
- In this video, Dr Ziad Ali shows how to measure diameter with an easy-to-use sizing algorithm.
Post-PCI Guidance: MAX | Medial dissection, Apposition, Xpansion are used to optimize stent placement to ensure optimal expansion.
Medial Dissection
There are three types of dissections: intimal, medial and intramural hematoma. A dissection which penetrates the medial layer and > 1 quadrant arc needs to be treated although various recommended angles exist, including > 60 degrees.9 A simplified approach used by operators is to measure a 1 quadrant arc.

Xpansion
An important aspect of optimizing PCI is the detection of underexpansion after stent placement.9
- Underexpansion is a predictor of adverse events (i.e. stent thrombosis and restenosis). Achieving optimal expansion is proven to reduce rates of adverse events.9
- In this video, Dr. Ziad Ali shows how to confirm stent expansion using OCT.

References
*As compared to AptiVue™ Software
- Reyes, M. The next innovation in PCI is not a stent. The value of OCT. CathLab Digest. Oct 6, 2019. Volume 27, Issue 10.
- Ali, Z. et al. Intracoronary optical coherence tomography: state of the art and future directions. EuroIntervention 2021;17:e105-e123. DOI: 10.4244/EIJ-D-21-00089
- AptiVue Software IFU. Refer to Instructions For Use (IFU) for additional information.
- Khuddus, M. et al. Cardiac Catheterization Laboratory Efficiency and Quality Improvement during Percutaneous Coronary Intervention (PCI) Utilizing a Standardized Optimal Coherence Tomography (OCT) Workflow in a Real-World Setting: Results from the LightLab Initiative. CRT 2021.
- Rauch A Standardized Optical Coherence Tomography Workflow Improves Procedural Efficiency and Safety During Percutaneous Coronary Intervention: Insights from the LightLab Clinical Initiative. TCT2021.
- Zhang J, et al. Intravascular ultrasound versus angiography-guided drug-eluting stent implantation: the ULTIMATE trial. J Am Coll Cardiol. 2018;72(24):3126-3137.
- Nef, Holger. OCT Compendium. Chapter 1. Systemic OCT image evaluation. First edition, 2016, Germany.
- Bezerra, H. et al: Analysis of changes in decision-making process during OCT-guided PCI -Insights from the LightLab Initiative. EuroPCR2020 Presentation.
- Räber L, et al. Clinical use of intracoronary imaging. Part 1: guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J. 2018;39(35):3281-3300.
- Prati, F. et al. The CLI-OPCI II Study. JACC: Cardiovascular Imaging, 2015: Vol 8, No. 11:1297-305.
References - MLD MAX graphic
- Fujino, A. et al. A new optical coherence tomography-based calcium scoring system to predict stent under expansion. EuroIntervention, April 2018; 13(18):e2182-e2189.
- Prati, F. et al. The CLI-OPCI II Study. JACC: Cardiovascular Imaging, 2015: Vol 8, No. 11:1297-305.
- Kubo, T. et al. Application of Optical Coherence Tomography in Percutaneous Coronary Intervention. Circulation Journal, September 2012: Vol. 76, 2076-2083.
- Ali, Z. et al. ILUMIEN III: Optimize PCI. Lancet 2016, 388:2618-2628.
- Souteyrand, G. et al. PESTO French Registry. European Heart Journal, 2016:37:1208-1216.
- Meneveau, N. et al. DOCTORS Study. Circulation, September 2016, 134:906-917.; Zhang, J. et al. The ULTIMATE Trial. Journal of the American College of Cardiology, Dec 2018: Vol 72, No 24:3126-37.; Russo, R. et al. The AVID Trial. Circ Cardiovasc Intervent, April 2009; 2:113-123.; De Jaegere, P. et al. MUSIC Study. European Heart Journal, February 1998:19,1214-1223.
MAT-2113908 v3.0
OPTIS™ and OPTIS™ Next Imaging Systems and Software

INDICATIONS
Applies to OPTIS™ Imaging Systems and Software
The OPTIS™ Software and AptiVue™ E Series Software are intended to be used only with compatible OPTIS™ Imaging Systems.
The OPTIS™ Imaging Systems with a compatible Dragonfly™ Imaging Catheter are intended for the imaging of coronary arteries and is indicated in patients who are candidates for transluminal interventional procedures. The compatible Dragonfly™ Imaging Catheters are intended for use in vessels 2.0 to 3.5 mm in diameter. The compatible Dragonfly™ Imaging Catheters are not intended for use in the left main coronary artery or in a target vessel which has undergone a previous bypass procedure.
The OPTIS™ Imaging Systems are intended for use in the catheterization and related cardiovascular specialty laboratories and will further compute and display various physiological parameters based on the output from one or more electrodes, transducers, or measuring devices. The physician may use the acquired physiological parameters, along with knowledge of patient history, medical expertise and clinical judgment to determine if therapeutic intervention is indicated.
Applies to OPTIS™ Next Imaging Systems and Software
The Ultreon™ 1.0 Software and Ultreon™ 2.0 Software are intended to be used only with compatible OPTIS™ Next Imaging Systems.
The OPTIS™ Next Imaging System with a compatible Dragonfly™ OPTIS™ Imaging Catheter or Dragonfly OpStar™ Imaging Catheter is intended for the imaging of coronary arteries and is indicated in patients who are candidates for transluminal interventional procedures. The Dragonfly™ OPTIS™ Imaging Catheter or Dragonfly OpStar™ Imaging Catheter is intended for use in vessels 2.0 to 3.5 mm in diameter. The Dragonfly™ OPTIS™ Imaging Catheter or Dragonfly OpStar™ Imaging Catheter is not intended for use in the left main coronary artery or in a target vessel which has undergone a previous bypass procedure.
The OPTIS™ Next Imaging Systems are intended for use in the catheterization and related cardiovascular specialty laboratories and will further compute and display various physiological parameters based on the output from one or more electrodes, transducers, or measuring devices. The physician may use the acquired physiological parameters, along with knowledge of patient history, medical expertise, and clinical judgment to determine if therapeutic intervention is indicated.
Applies to both OPTIS™ and OPTIS™ Next Imaging Systems and Software
The Dragonfly™ OPTIS™ or Dragonfly™ OpStar™ Imaging Catheters are intended for use in vessels 2.0 to 3.5 mm in diameter. The Dragonfly™ OPTIS™ or Dragonfly™ OpStar™ Imaging Catheters are not intended for use in the left main coronary artery or in a target vessel which has undergone a previous bypass procedure.
The OPTIS™ and OPTIS™ Next Imaging Systems are intended for use in the catheterization and related cardiovascular specialty laboratories and will further compute and display various physiological parameters based on the output from one or more electrodes, transducers, or measuring devices. The physician may use the acquired physiological parameters, along with knowledge of patient history, medical expertise, and clinical judgment to determine if therapeutic intervention is indicated.
CONTRAINDICATIONS
The OPTIS™ and OPTIS™ Next Integrated Systems and Mobile Systems with the usage of the OPTIS™ Software, AptiVue™ E Series Software, Ultreon™ 1.0 Software, and Ultreon™ 2.0 Software are contraindicated where introduction of any catheter would constitute a threat to patient safety. Contraindications include:
- Bacteremia or sepsis
- Major coagulation system abnormalities
- Patients diagnosed with coronary artery spasm
- Patients disqualified for coronary artery bypass graft (CABG) surgery
- Patients disqualified for percutaneous transluminal coronary angioplasty (PTCA)
- Severe hemodynamic instability or shock
- Total occlusion
- Large thrombus
- Acute renal failure
- Inability to tolerate systemic anticoagulation is a contraindication to use of OCT for coronary imaging.
- The system has no patient alarm functions. Do not use for cardiac monitoring.
COMPLICATIONS
The following complications may occur as a consequence of intravascular imaging and catheterization procedure:
- Abnormal heart rhythm or arrhythmias
- Acute myocardial infarction
- Allergic reaction to the contrast media or drug administered for the procedure
- Arterial dissection, injury, or perforation
- Bleeding
- Catheter access site reactions: inflammation or granuloma
- Coronary artery spasm
- Death
- Embolism
- Hypotension
- Infection
- Myocardial ischemia
- Renal insufficiency or failure from contrast media use
- Repeat revascularization
- Thrombus formation, abrupt closure, or total occlusion
- Tissue necrosis
- Unstable angina
WARNINGS
- Prior to use, please review the Instructions for Use supplied with the OPTIS™ imaging system, Dragonfly™ Imaging Catheter, Wi-Box™ AO Transmitter and the PressureWire™ guidewire for more information.
- The Dragonfly™ Imaging Catheter is sterilized by ethylene oxide and is intended for one time use only. Non-pyrogenic. Do not use if the package is opened or damaged. Do not reuse or re-sterilize. Any attempt to reuse or re-sterilize may compromise the structural integrity of this device. Adverse effects of using a non-sterile or re-sterilized catheter may include, but are not limited to: local and / or systemic infection, mechanical damage, inaccurate results.
- Appropriate anticoagulant and vasodilator therapy must be used during the procedure as needed.
- Ensure that no air is introduced into the system during the Dragonfly™ Imaging Catheters insertion.
- Observe all advancement and movement of the Dragonfly™ Imaging Catheters under fluoroscopy. Always advance and withdraw the catheter slowly. Failure to observe device movement fluoroscopically may result in vessel injury or device damage. To ensure proper placement, do not move the guide wire after a Dragonfly™ Imaging Catheter is in place.
- If resistance is encountered during advancement or withdrawal of the Dragonfly™ Imaging Catheter, stop manipulation and evaluate under fluoroscopy. If the cause of resistance cannot be determined or mitigated, carefully remove the Dragonfly™ Imaging Catheters and guidewire together as a unit from the patient.
- Leave the guide wire engaged with a Dragonfly™ Imaging Catheter at all times during use. Do not withdraw or advance the guide wire prior to withdrawing the Dragonfly™ Imaging Catheters.
- The Dragonfly™ Imaging Catheters should never be forced into lumens that are narrower than the Dragonfly™ Imaging Catheters body or forced through a tight or heavily calcified lesion.
- The Dragonfly™ Imaging Catheters should not be advanced through abnormally tortuous anatomy.
- When advancing or retracting a Dragonfly™ Imaging Catheter with a monorail tip through a stented vessel, the Dragonfly™ Imaging Catheters may engage the stent between the junction of the Dragonfly™ Imaging Catheters and guide wire, resulting in entrapment of catheter / guide wire, catheter tip separation, stent dislocation, and / or vascular injury.
- Refer to the contrast media Instructions for Use for general warnings and precautions relating to use of contrast media.
- Before creating an OCT recording, review “Performing an OCT Procedure” for additional warnings and cautions in the IFU.
PRECAUTIONS
- Safety and effectiveness have been established for the following patient population: adult patients undergoing non-emergent percutaneous coronary interventions in lesions with reference vessel diameters between 2.0 to 3.5 mm, which are not located in the left main coronary artery or in a target vessel which has undergone previous bypass procedures.
- Follow all instructions, warnings, and cautions provided in “Patient Safety” in the IFU.
- All operators must be knowledgeable in performing OCT and physiological procedures prior to using the OPTIS™ and OPTIS™ Next Integrated Systems and Mobile Systems with the usage of the OPTIS™ Software, AptiVue™ E Series Software, Ultreon™ 1.0 Software, and Ultreon™ 2.0 Software.
- When using saline, heparinized saline is recommended.
- Monitor the OCT image for indications of the Dragonfly™ Imaging Catheters optical failure. If optical failure is suspected, remove the Dragonfly™ Imaging Catheter from the patient, press “Unload” on the drive motor and optical controller (DOC), detach the catheter, and replace it with a new one.
- If the pullback triggers before contrast is injected, repeat the pullback.
- For optimal imaging, only use 100% contrast media.
- Use the minimum flush rate and volume required to image the desired anatomy.
- To obtain accurate measurements, be sure the selection for the Flush Medium is the same as the medium in which you are imaging.
- The Dragonfly™ Imaging Catheters must be purged prior to connection to the DOC to prevent damage to the imaging core.
- Do not insert or remove a Dragonfly™ Imaging Catheter while the DOC is scanning. Do not attempt to disconnect the catheter from the DOC while the “lock” LED is blinking as it could damage the catheter or the DOC. Refer to “Removing the Dragonfly™ Imaging Catheter” in the IFU.
- Never attempt to attach or detach a catheter to the DOC while the "lock" LED is lit.
- Take care in handling the Dragonfly™ Imaging Catheters to prevent breaking the fiber-optics within the catheter. Kinking and bending of the catheter can cause damage. While connecting, ensure the proximal catheter segment is straight and aligned with the DOC. Never attempt to connect and operate the catheter while the catheter remains coiled within the hoop.
- Do not kink, sharply bend, pinch, or crush the Dragonfly™ Imaging Catheters at any time.
- The Dragonfly™ Imaging Catheters have no user serviceable parts. Do not attempt to repair or alter any part of the catheter assembly as provided.
- If you want to make measurements on files that will be exported to standard formats, you must make the measurements BEFORE exporting the images. Using non-OCT software to measure standard format images will not produce accurate measurements.
- Do not use images that have been exported to JPEG or Compressed AVI formats for clinical decision making. These formats use compression methods that may degrade the image quality.
- Artifacts may result in misrepresentation of L-mode data, so L-mode is not recommended for quantification of clinical information.
- It is the user’s responsibility to confirm the lumen contours of all the frames within the reference segment, and to make adjustments if necessary. Red frames indicate low confidence in the detected contours.
- Deleted files cannot be restored. After files have been deleted, they can only be imported back to your system from your archived copies.
- Restoring factory default settings resets ALL user-entered configuration values except the date and time. This button should be used only under the direction of qualified service personnel.
MAT-2309288 v1.0
Dragonfly OpStar™ Imaging Catheter
Indications: The Dragonfly OpStar™ Imaging Catheter with the OCT Imaging System is intended for the imaging of coronary arteries and is indicated in patients who are candidates for transluminal interventional procedures. The Dragonfly OpStar™ Imaging Catheter is intended for use in vessels 2.0 to 3.5 mm in diameter. The Dragonfly OpStar™ Imaging Catheter is not intended for use in the left main coronary artery or in a target vessel which has undergone a previous bypass procedure.
Contraindications: Use of the Dragonfly OpStar™ Imaging Catheter is contraindicated where introduction of any catheter would constitute a threat to patient safety. Contraindications include:
- Acute renal failure
- Bacteremia or sepsis
- Large thrombus
- Major coagulation system abnormalities
- Patients diagnosed with coronary artery spasm
- Patients disqualified for coronary artery bypass graft (CABG) surgery
- Patients disqualified for percutaneous transluminal coronary angioplasty (PTCA)
- Severe hemodynamic instability or shock
- Total occlusion
- Inability to tolerate systemic anticoagulation is a contraindication to use of OCT for coronary imaging
Warnings:
- Appropriate anticoagulant and vasodilator therapy is recommended to be used during the procedure as ordered by the physician.
- The Dragonfly OpStar™ Imaging Catheter is sterilized by ethylene oxide and is intended for one time use only. Nonpyrogenic. Do not use if the package is opened or damaged. Do not reuse or re-sterilize. Any attempt to reuse or re-sterilize may compromise the structural integrity of this device. Adverse effects of using a non-sterile or re-sterilized imaging catheter may include, but are not limited to:
- Local and/or systemic infection
- Mechanical damage
- Inaccurate results
- Note the product "Use by" date on the package.
- Observe all advancement and movement of the Dragonfly OpStar™ Imaging Catheter under fluoroscopy. Always advance and withdraw the catheter slowly and ensure that the guide wire is coaxial to the monorail. Failure to observe device movement fluoroscopically may result in vessel injury or device damage. To ensure proper placement, do not move the guide wire after the Dragonfly OpStar™ Imaging Catheter is in place.
- If resistance is encountered during withdrawal of the Dragonfly OpStar™ Imaging Catheter:
- Stop manipulation and evaluate under fluoroscopy.
- If guide wire prolapse is observed, readvance the catheter, ensure the guide wire is coaxial - to the monorail, and reattempt withdrawal.
- If the cause of resistance cannot be determined or mitigated, carefully remove the Dragonfly OpStar™ Imaging Catheter and guide wire as a unit from the patient and replace the Dragonfly OpStar™ Imaging Catheter and guide wire. Do not reuse the Dragonfly OpStar™ Imaging Catheter and guide wire.
- Leave the guide wire engaged with the Dragonfly OpStar™ Imaging Catheter at all times during use. Do not retract or advance the guide wire prior to withdrawing the Dragonfly OpStar™ Imaging Catheter.
- The Dragonfly OpStar™ Imaging Catheter should never be forced into lumens that are narrower than the catheter body or forced through a tight or heavily calcified lesion.
- The Dragonfly OpStar™ Imaging Catheter should not be advanced through abnormally tortuous anatomy.
- When advancing or retracting a Dragonfly OpStar™ Imaging Catheter with a monorail tip through a stented vessel, the Dragonfly imaging catheter may engage the stent between the junction of the Dragonfly OpStar™ Imaging Catheter and guide wire, resulting in entrapment of the catheter/guide wire, catheter tip separation, stent dislocation and/or vascular injury.
- Do not remove the Dragonfly OpStar™ Imaging Catheter from the DOC until the procedure is complete to avoid a potential sterility breach.
- Always verify that the Dragonfly OpStar™ Imaging Catheter has been properly prepared prior to inserting into vasculature.
- The safety and effectiveness of the coated device has not been established, or is unknown, in vascular regions other than those specifically indicated.
- Failure to abide by the warnings in this Instructions for Use might result in damage to the device coating, which may necessitate intervention or result in serious adverse events.
Precautions:
- Safety and effectiveness have been established for the following patient population: adult patients undergoing non-emergent percutaneous coronary interventions in lesions with reference vessel diameters between 2.0 mm to 3.5 mm, which were not located in the left main coronary artery or in a target vessel which has undergone a previous bypass procedure.
- Use the minimum flush rate and volume required to image the desired anatomy.
- For optimal imaging, only use 100% contrast media.
- Refer to contrast media Instructions for Use for general warnings and precautions relating to contrast media.
- Do not kink, sharply bend, pinch, or crush the Dragonfly OpStar™ Imaging Catheter at any time.
- The Dragonfly OpStar™ Imaging Catheter has no user serviceable parts. Do not attempt to repair or alter any part of the Dragonfly OpStar™ Imaging Catheter assembly as provided.
- After use, the Dragonfly OpStar™ Imaging Catheter may be a potential biohazard. Handle and dispose of in accordance with accepted medical practice and applicable laws and regulations.
- When using saline, heparinized saline is recommended. When wet, the hydrophilic coating increases the lubricity of the coated surface.
- Avoid abrasion of the hydrophilic coating. Use caution when manipulating, advancing and / or withdrawing these devices through needles, metal cannulas, stents, or other devices with sharp edges, or through tortuous or calcified blood vessels. Manipulation, advancement, and / or withdrawal past sharp or beveled edges may result in destruction and / or separation of the outer coating, which may lead to clinical adverse events, resulting in coating material remaining in the vasculature or device damage. This may result in adverse events requiring additional intervention.
- The integrity and performance of the device coating can be negatively impacted by preparation with incompatible media or solvents. Please take note of the following important recommendations:
- Avoid wiping the device with dry gauze as this may damage the device coating.
- Avoid excessive wiping of the coated device.
- Avoid using alcohol, antiseptic solutions, or other solvents to pre-treat the device because this may cause unpredictable changes in the coating which could negatively affect the safety and performance of the catheter.
- Do not soak the device as it may adversely impact the hydrophilic coating on the catheter.
- The Dragonfly OpStar™ Imaging Catheter must be purged prior to connection to the DOC to prevent damage to the imaging core.
- Ensure that the Dragonfly OpStar™ Imaging Catheter tip marker has been properly identified and differentiated from the lens marker before contrast administration and prior to performing the OCT reading.
- Never attempt to attach or detach the Dragonfly OpStar™ Imaging Catheter to the DOC while the "lock" LED is lit.
Complications:
The following complications may occur as a consequence of intravascular imaging and catheterization procedure:
- Allergic reaction to the contrast media or drug administered for the procedure
- Bleeding
- Arterial dissection, injury or perforation
- Abnormal heart rhythm or arrhythmias
- Unstable angina
- Coronary artery spasm
- Thrombus formation, abrupt closure, or total occlusion
- Embolism
- Infection
- Myocardial ischemia
- Acute myocardial infarction
- Repeat revascularization
- Renal insufficiency or failure from contrast media use
- Death
- Catheter access side reactions: inflammation or granuloma or tissue necrosis
- Hypotension
MAT-2115499 v4.0