
XIENCE™ Stent Clinical Outcomes
Stent choice matters. And a wealth of clinical evidence supports the safety of the XIENCE™ Stent, which is why experts consider XIENCE™ Stent to be the gold standard among DES.1
In addition, reproducible procedural outcomes are a proven quality of XIENCE™ DES performance,2 delivering consistent patient safety with low complication rates3
When choosing XIENCE™ Stent, interventional cardiologists (ICs) can know that the optimal outcomes they achieved in the cath lab will persist far into the future—not only treating stenosed vessels but enabling patients to have a better quality of life.4
There’s a Whole World of Evidence to Support the XIENCE™ Stent
XIENCE™ Stent is the world's leading DES, with over 20 million implants.5




Substantial clinical data continue to provide evidence that XIENCE™ DES can effectively treat a broad spectrum of patients.1 Given the best in class deliverability and the expanded treatment options of XIENCE Skypoint™ Stent,7 it is an excellent choice for complex patients.
Key XIENCE™ Stent Clinical Trials
XIENCE 28 & XIENCE 90 Data
XIENCE™ Stent with either 1-month or 3-month Dual Antiplatelet Therapy (DAPT) reduced severe bleeding with no increase in ischemic events.8
Short DAPT: Reduced Severe Bleeding8
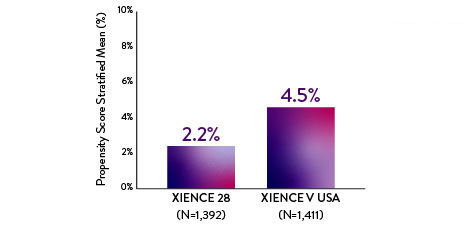
XIENCE 28: BARC 3-5 BLEEDING
Between 1 and 6 months
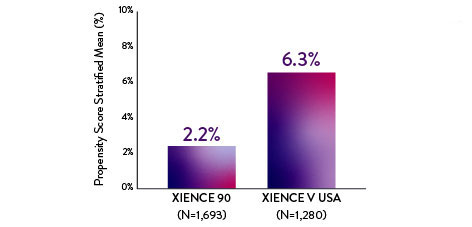
XIENCE 90: BARC 3-5 BLEEDING
Between 3 and 12 months
Note: PS stratified analysis for BARC 3-5 bleeding was not pre-specified.
Note: BARC 2-5 was a powered secondary endpoint.
Short DAPT: No Increase in Ischemic Events in High Bleeding Risk (HBR) Patients8
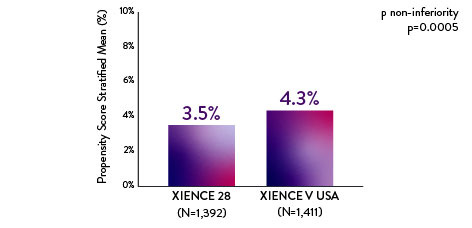
XIENCE 28: 1-month DAPT in HBR Patients
XIENCE 28: All Deaths or MI
Between 1 and 6 months
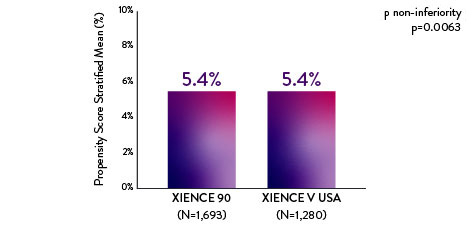
XIENCE 90: 3-month DAPT in HBR Patients
XIENCE 90: All Deaths or MI
Between 3 and 12 months
NOTE: Antiplatelet drugs should be used in combination with the XIENCE stent, per the guidelines from the American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions (ACC/AHA/SCAI). DAPT regimen is at the discretion of the physician and dependent on individual patient needs. Data from the short DAPT program, XIENCE 28, showed that 1-month DAPT (as short as 28 days) duration post-PCI is safe for HBR patients.
CARDIOBASE Registry Data: XIENCE™ Stent vs Synergy‡
XIENCE™ Stent vs Synergy‡ with short-term safety outcomes in real-world patients.9
Short-Term Data with XIENCE™ Stent and Synergy‡
XIENCE™ Stent: Significantly Lower Acute Definite Stent Thrombosis vs Synergyǂ9
75% Less acute definite stent thrombosis with XIENCE™ Stent System compared to Synergyǂ
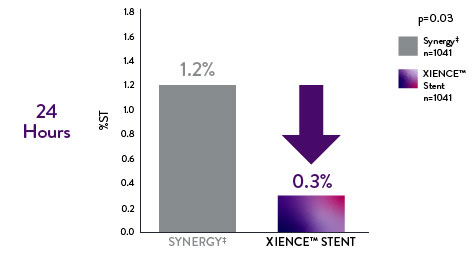
Propensity-matched analysis from a single-center registry.
XIENCE™ Stent: Significantly Lower Target Lesion Revascularization (TLR) at 1 Month vs Synergyǂ9
Suggests favorable economic benefits* for XIENCE Stent vs. Synergyǂ in clinical practice
*Driven by reduction in additional procedures and hospitalizations
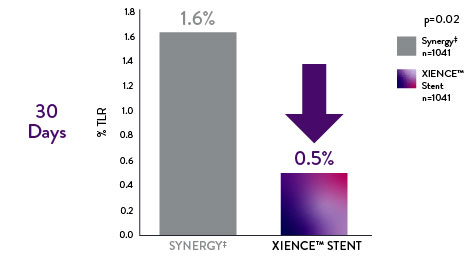
Target Lesion Revascularization
RESOLUTE All-Comers (RAC) Randomized Trial Data: XIENCE™ Stent vs Resolute‡
Safety data from RAC real-world patients also reveal that XIENCE™ Stent outperforms Resolute.‡10
XIENCE™ Stent: Significantly Lower Early Definite Stent Thrombosis vs Resoluteǂ10
88% less definite stent thrombosis with XIENCE™ Stent compared to Resoluteǂ
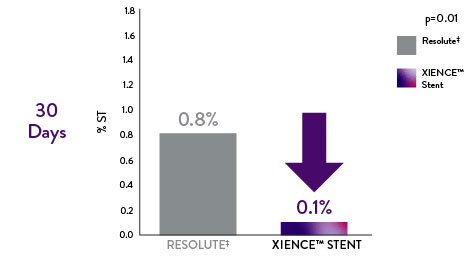
Definite Stent Thrombosis
XIENCE™ Stent: Significantly Lower Late Definite Stent Thrombosis vs Resoluteǂ11
75% less definite stent thrombosis with XIENCE™ Stent compared to Resoluteǂ
Note: Primary endpoint for non-inferiority was met by Resoluteǂ compared with XIENCE™ Stent. The primary endpoint of target lesion failure (TLF) was a composite of cardiac death, myocardial infarction, and clinically indicated target lesion revascularization at 12 months.
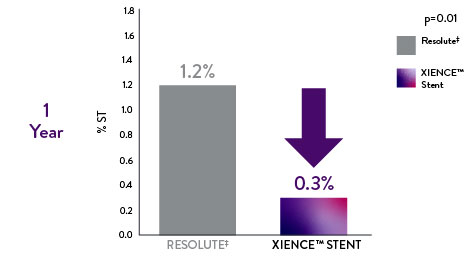
Definite Stent Thrombosis
References:
- Zanchin C, et al. JACC Cardiovasc Interv. 2019;12(17):1665-1675. Serruys P, et al. N Engl J Med. 2010;363:136-146. Shiomi H, et al. JACC Cardiovasc Interv. 2019;12:637-647. Kufner S, et al. Circulation. 2019:139(3):325-333. Palmerini T, et al. Lancet. 2013;379:1393-1402. Bangalore S, et al. Circulation. 2012;125:2873-2891. Bangalore S, et al. Circ Cardiovasc Interv. 2013;6(6):378-390. Pilgrim T, et al. Lancet. 2014;384:2111-2122. Pilgrim T, et al. Lancet. 2018;392:737-746. Data on file at Abbott.
- Saito S, et al. Eur Heart J. 2014;35:2021-2031. Saito S, et al. EuroIntervention. 2019;15(11):e1006-e1013. Natsuaki M, et al. J Am Coll Cardiol. 2013;62:181-190. Stone G, et al. Lancet 2018;392:1530-1540.
- Zanchin C, et al. JACC Cardiovasc Interv. 2019;12(17):1665-1675. Serruys P, et al. N Engl J Med. 2010;363:136-146. Shiomi H, et al. JACC Cardiovasc Interv. 2019;12:637-647. Kufner S, et al. Circulation. 2019:139(3):325-333.
- Baron SJ, et al. J Am Coll Cardiol. 2017;70:3113-3122.
- Data on file at Abbott. 20 million implants is based on DES data through Q4, 2022.
- Kufner S, et al. Circulation. 2019:139(3):325-333.
- Data on file at Abbott. XIENCE Skypoint (TM) Stent Instructions for Use (IFU). Refer to IFU for additional information.
- XIENCE Skypoint™ Stent – Instructions for Use
- Zanchin C. et al. JACC Cardiovasc Interv. 2019;12(17):1665-1675.
- Serruys P, et al. N Engl J Med. 2010;363:136-146.
MAT-2414811 v1.0
XIENCE Skypoint™, XIENCE Sierra™, XIENCE Alpine™ (XIENCE™ Family) Everolimus Eluting Coronary Stent Systems

Indications
Applies to XIENCE Skypoint™ Stent Systems:
- Indicated for improving coronary artery luminal diameter in patients, including those with diabetes mellitus, with symptomatic heart disease due to de novo native coronary artery lesions ≤ 44 mm in length with reference vessel diameters of ≥ 2.25 mm to ≤ 5.25 mm and for high bleeding risk patients with coronary arteries lesions ≤ 32 mm in length with a reference vessel diameter of ≥ 2.25 mm and ≤ 5.25 mm.
- Treating de novo chronic total coronary occlusions.
Applies to XIENCE Sierra™ and XIENCE Alpine™ Stent Systems:
- Indicated for improving coronary artery luminal diameter in patients, including those at high risk for bleeding and those with diabetes mellitus, with symptomatic heart disease due to de novo native coronary artery lesions (length ≤ 32 mm) with reference vessel diameters of ≥ 2.25 mm to ≤ 4.25 mm.
- Treating de novo chronic total coronary occlusions.
Contraindications
The XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems are contraindicated for use in:
- Patients who cannot tolerate, including allergy or hypersensitivity to, procedural anticoagulation or the post-procedural antiplatelet regimen.
- Patients with hypersensitivity or contraindication to everolimus or structurally-related compounds, or known hypersensitivity to stent components (cobalt, chromium, nickel, tungsten, methacrylic polymer, fluoropolymer), or with contrast hypersensitivity.
Warnings
- Each stent and the delivery system are for single use only. Do not reuse, reprocess, or resterilize. Note the product “Use by” date on the package. Reuse, reprocessing, or resterilization may compromise the structural integrity of the device and / or delivery system and / or lead to device failure, which may result in patient injury, illness, or death. Reuse, reprocessing, or resterilization may also create a risk of contamination of the device and / or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device and / or delivery system may lead to injury, illness, or death of the patient.
- It is not recommended to treat patients having a lesion that prevents complete inflation of an angioplasty balloon.
- Antiplatelet therapy should be administered post-procedure.
- This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
- Judicious selection of patients is necessary, since the use of this device carries the associated risk of stent thrombosis, vascular complications, and/or bleeding events.
- The XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems are coated with an everolimus and polymer coating at the full implant stent length. The distal and intermediate portions of the device, the tip, and tapers of the balloon are coated with HYDROCOAT™ Hydrophilic Coating.
Failure to abide by the warnings in this labeling might result in damage to the device coating, which may necessitate intervention or result in serious adverse events.
Precautions
- Implantation of the stent should be performed only by the physicians who have received appropriate training.
- Stent placement should be performed at centers where emergency coronary artery bypass graft surgery (CABG) can be readily performed.
- When the XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems are used outside the specified Indications for Use, patient outcomes may differ from the results observed in the SPIRIT family of clinical trials. Compared to use within the specified indications for use, the use of the XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems in patients and lesions outside of the labeled indications, including more tortuous anatomy, may have an increased risk of adverse events, including stent thrombosis, stent embolization, MI, or death.
- The extent of the patient’s exposure to drug and polymer is directly related to the number of stents implanted. See Instructions for Use for current data on multiple stent implantation.
- Safety and effectiveness of the XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems have not been established for subject populations with the following clinical settings:
- Patients with prior brachytherapy of the target lesion or the use of brachytherapy for treated site restenosis.
- Conjunctive use of the XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems with either mechanical atherectomy devices or laser angioplasty catheters.
- Women who are pregnant or lactating, men intending to father children, pediatric.
- Unresolved vessel thrombus at the lesion site, coronary artery reference vessel diameters < 2.25 mm or > 4.25 mm, for XIENCE Skypoint™ < 2.25 mm or > 5.25 mm, or lesion lengths >44 mm, lesions located in saphenous vein grafts, lesions located in unprotected left main coronary artery, ostial lesions, or lesions located at a bifurcation or previously stented lesions, diffuse disease or poor flow (TIMI < 1) distal to the identified lesions, excessive tortuosity proximal to or within the lesion, recent Acute Myocardial Infarction (AMI) or evidence of thrombus in target vessel, multivessel disease, and in-stent restenosis.
- Formal drug interaction studies have not been performed with the XIENCE Skypoint™, XIENCE Sierra™ or XIENCE Alpine™ Stent Systems because of limited exposure to everolimus eluted from XIENCE Skypoint™, XIENCE Sierra™ and XIENCE Alpine™ Stent Systems.
- Everolimus, the active ingredient in the stents, is an immunosuppressive agent. Consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression.
- Oral everolimus use in renal transplant and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglyceride levels, which in some cases required treatment.
- Nonclinical testing has demonstrated that the XIENCE Sierra™ and XIENCE Alpine™ Stent Systems in single and in overlapped configurations up to 71 mm, for XIENCE Skypoint™ 91 mm in length, are MR Conditional. See Instructions for Use for detailed scanning conditions
Potential Adverse Events
Adverse events that may be associated with PCI treatment procedures and the use of a stent in native coronary arteries include, but are not limited to, the following:
- Allergic reaction or hypersensitivity to latex, contrast agent anesthesia, device materials, and drug reactions to everolimus, anticoagulation, or antiplatelet drugs
- Vascular access complications which may require transfusion or vessel repair, including: Catheter site reactions, Bleeding, Arteriovenous fistula; pseudoaneurysm, aneurysm, dissection, perforation/rupture, Embolism, Peripheral nerve injury, Peripheral ischemia
- Coronary artery complications which may require additional intervention, including: Total occlusion or abrupt closure, Arteriovenous fistula, pseudoaneurysm, aneurysm, dissection. Perforation/rupture, Tissue prolapse/plaque shift, Embolism, Coronary or stent thrombosis, Stenosis or restenosis
- Pericardial complications which may require additional intervention, including: Cardiac tamponade, Pericardial effusion, Pericarditis.
- Cardiac arrhythmias
- Cardiac ischemic conditions (including myocardial ischemia, myocardial infarction (including acute), coronary artery spasm, and unstable or stable angina pectoris)
- Stroke/Cerebrovascular Accident (CVA) and Transient Ischemic Attack (TIA)
- System organ failures: Cardio-respiratory arrest, Cardiac failure, Cardiopulmonary failure, Renal Insufficiency/failure, Shock
- Bleeding
- Blood cell disorders
- Hypotension and/or hypertension
- Infection
- Nausea and vomiting
- Palpitations
- Dizziness
- Syncope
- Chest Pain
- Fever
- Pain
- Death
The risks described below include the anticipated adverse events relevant for the cardiac population referenced in the contraindications, warnings and precaution sections of the everolimus labels / SmPCs and / or observed at incidences ≥ 10% in clinical trials with oral everolimus for different indications. Please refer to the drug SmPCs and labels for more detailed information and less frequent adverse events.
- Abdominal pain
- Anemia
- Angioedema
- Arterial Thrombotic Events
- Bleeding and coagulopathy
- Constipation
- Cough
- Diabetes mellitus
- Diarrhea
- Dyspnea
- Embryo-fetal toxicity
- Erythema
- Erythroderma
- Headache
- Hepatic artery thrombosis
- Hepatic disorders
- Hypersensitivity to everolimus active substance, or to other rapamycin derivates
- Hypertension
- Infection (bacterial, fungal, viral or protozoan infections, including infections with opportunistic pathogens). Polyoma virus-associated nephropathy (PVAN), JC virus-associated progressive multiple leukoencephalopathy (PML), fatal infections and sepsis have been reported in patients treated with oral everolimus
- Kidney arterial and venous thrombosis
- Laboratory test alterations
- Lymphoma and skin cancer
- Male infertility
- Menstrual irregularities
- Nausea
- Nephrotoxicity
- Non-infectious pneumonitis
- Oral ulcerations
- Pain
- Pancreatitis
- Pericardial effusion
- Peripheral edema
- Pleural effusion
- Pneumonia
- Pyrexia
- Rash
- Renal Failure
- Upper respiratory tract infection
- Urinary tract infection
- Venous thromboembolism
- Vomiting
- Wound healing complications
There may be other potential adverse events that are unforeseen at this time.
MAT-2100879 v7.0