
Epicardial Assessment with FFR, RFR, and PPG
Epicardial physiology indices such as Fractional Flow Reserve (FFR), Resting Full-cycle Ratio (RFR) and Pullback Pressure Gradient (PPG) are utilized to determine the need and predict the likelihood of successful percutaneous coronary intervention (PCI).
FFR or RFR assessments are performed to assess the functional significance of epicardial coronary lesions at stress or rest, respectively.1 PPG is a novel epicardial index that objectively quantifies focal epicardial disease to identify patients that are most likely to benefit from PCI.
Measure FFR, RFR, and PPG with PressureWire™ X Guidewire, the world's only2,3 wireless physiology wire with a hydrophilic-coated3 design for exceptional handling performance and accurate, reliable readings.4,5
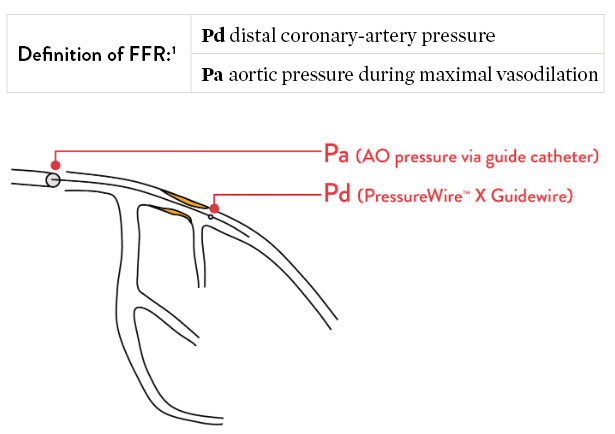
FFR: Fractional Flow Reserve
Measuring FFR
FFR is a measure of blood pressure difference across a coronary artery stenosis to determine if a stenosis is physiologically significant, which can impede oxygen delivery to the heart muscle.1
FFR is the gold standard of assessing a functionally significant coronary stenosis.6,7
Why Use FFR?
34%
of the time angiography is inaccurate
Coronary angiography is not accurate in guiding the functional significance of stenosis in 34% of cases, compared to FFR.8
35%
risk reduction in death/MI with FFR
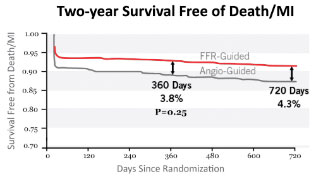
FFR-guided percutaneous coronary intervention (PCI) leads to a 35% risk reduction in death and myocardial infarction (MI), compared to relying only on angiography.9
62%
relative risk reduction in MACCE
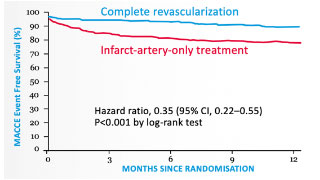
Complete revascularization with PressureWire™ X Guidewire led to a 62% relative risk reduction in major adverse cardiac and cerebrovascular events (MACCE) at 1 year.10 The DANAMI-3-PRIMULTI trial also revealed that untreated “FFR-positive” non-infarct-related artery lesions are associated with a 31% incidence of MACCE at 1 year.10
RFR: Resting Full-Cycle Ratio
PressureWire™ X Guidewire measures RFR, a resting index that can be measured as an alternative to FFR depending on the clinical situation.11 Like FFR, RFR can identify functionally significant epicardial coronary stenosis. Unlike FFR, RFR is a non-hyperemic index that does not require the administration of a vasodilator such as adenosine.11
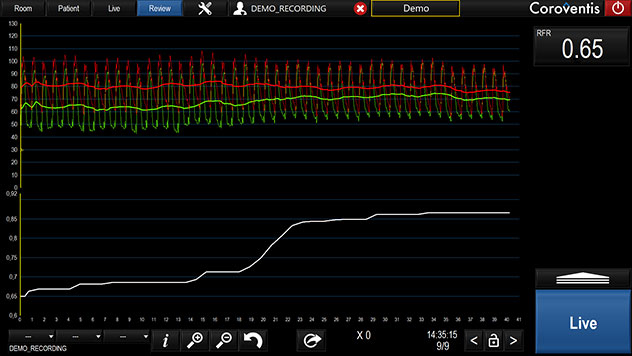
Measuring RFR
Clinically equivalent to the instantaneous wave-free ratio (iFR‡) resting index, Abbott's RFR resting index scans through diastole and systole for the lowest pd/pa ratio. Unlike iFR‡ or diastolic pressure ratio (dPR‡), RFR is calculated from the lowest value of Pd/Pa over the entire cardiac cycle.12
Advantage of RFR
"The major advantage of RFR over iFR‡ is that RFR does not require identification of a specific landmark or selection of a specific time point during diastole. By calculating the minimum Pd/Pa over the entire cardiac cycle, RFR calculates the maximum pressure gradient across the stenosis during resting status."
– Lee, et al. Circulation 2019
The cutoff value of RFR is 0.89:11,13,14
- When RFR ≤ 0.89, treatment with percutaneous coronary intervention (PCI) may be beneficial
- When RFR > 0.89, deferral of PCI may be beneficial
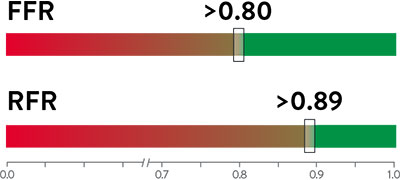
Green indicates deferral of PCI may be beneficial, and red indicates a treatment of PCI may be beneficial.
Assessing Serial or Diffuse Lesions with RFR Pullback
In patients with multiple sequential stenoses or diffuse lesions, pullback pressure assessment can identify lesions with functional significance. RFR can be calculated along the entire length of a stenotic vessel using pullback, which measures pressure gradient at any given location.11
RFR Compared to Other Resting Indices
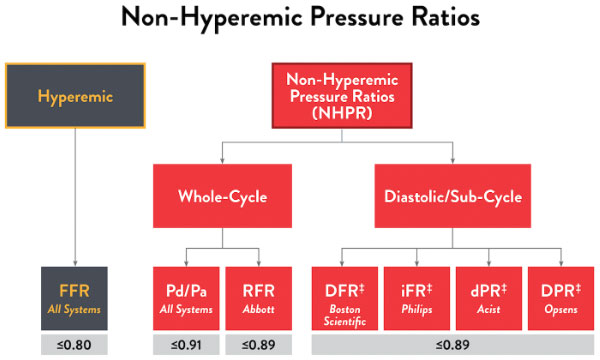
All resting pressure-derived indices closely correlate with one another, revealing the same discriminatory ability to guide intervention.12 The large IRIS-FFR retrospective study (1,506 patients, 1,833 lesions) examined deferred lesion failure among 5 resting indices—resting Pd/Pa, iFR‡, RFR, dPR‡, and DFR‡—and concluded that all resting indices had similar outcomes in deferred lesions.14
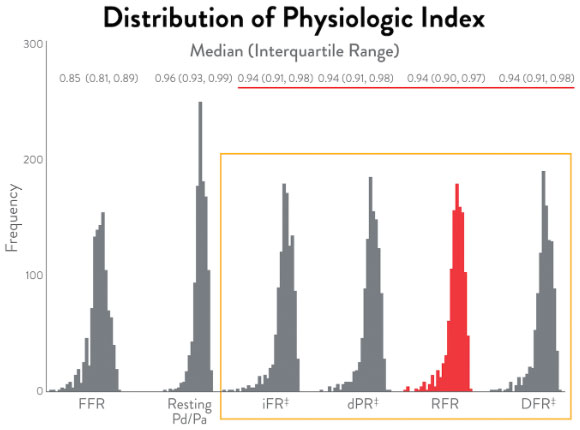
Here are the cutoff values for the various non-hyperemic pressure ratios.16
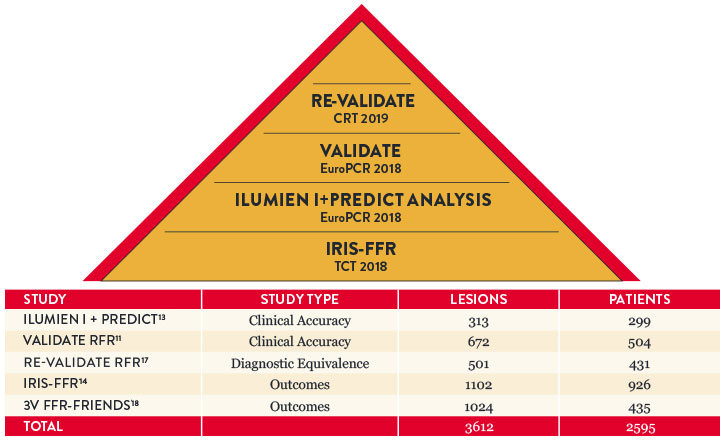
Key RFR Findings
RFR has been studied in over 3,500 lesions and 2,500 patients, showing clinical accuracy and outcomes.
Objective Decision Making: Drift Matters
Drift is a phenomenon that affects the accuracy of most pressure measurement devices.19 Accuracy is particularly critical for resting ratios, as clinical decisions from resting ratios are more impacted by drift than FFR.20,21
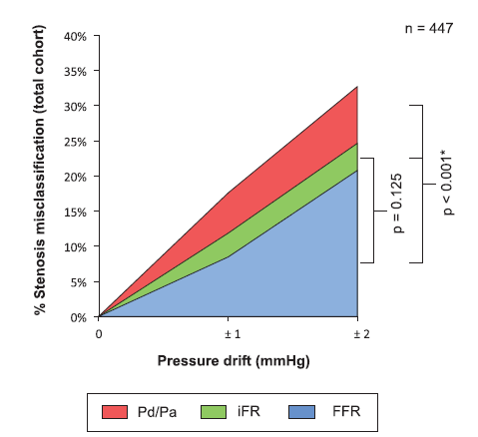
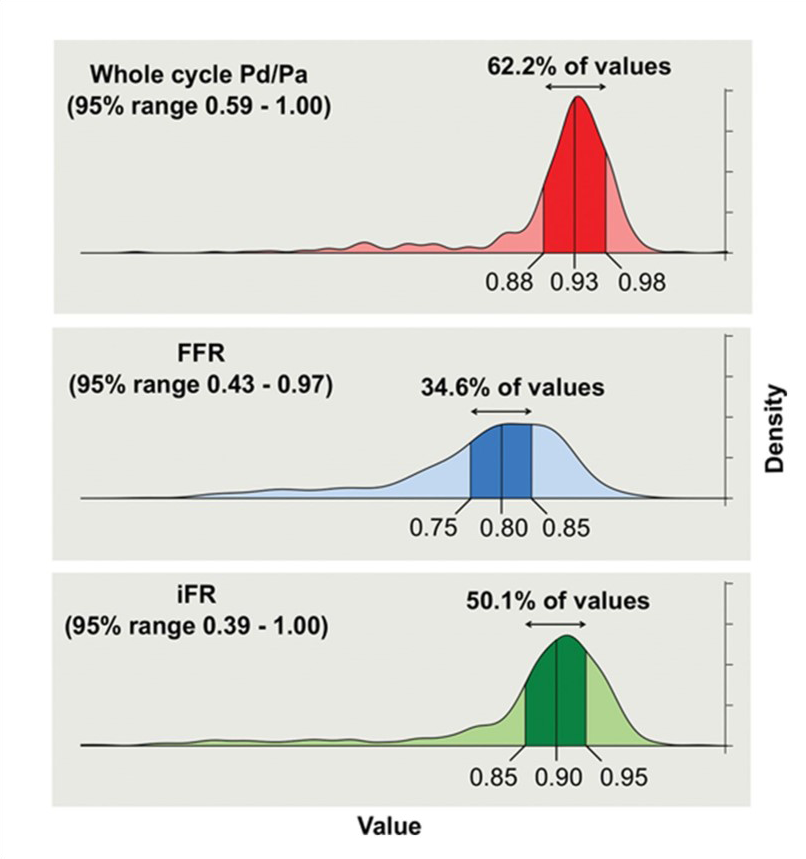
Compared to the hyperemic state, smaller separation between Pd and Pa at rest means even relatively small amounts of drift can lead to stenosis misclassification compared to FFR. That’s why it critical to detect even the slightest difference of pressure.
Use of FFR vs RFR16
| Uses of FFR | RFR | FFR |
|---|---|---|
| Left Main Coronary Artery22 | – | +++ |
| Systolic Dysfuntion23 | – | +++ |
| Post-PCI Side Branch Interrogation24 | – | +++ |
| Post-PCI Assessment25 | – | +++ |
| Equivalent Assessment | ||
| Multi-Vessel Disease26 | +++ | +++ |
| Diabetes27 | +++ | +++ |
| Uses of RFR | ||
| Tandem Lesions28 | +++ | + |
| Diffuse Lesions29 | +++ | + |
| Left Anterior Descending30 | +++ | ++ |
| Acute Coronary Syndrome31 | +++ | ++ |
Chart courtesy of Ziad Ali, MD.
PPG: Pullback Pressure Gradient
PPG is a predictive tool that quantifies focal coronary disease to enable precise PCI decision-making for better patient outcomes.32-36
Why Measure PPG?
Enhance Actionable Insights
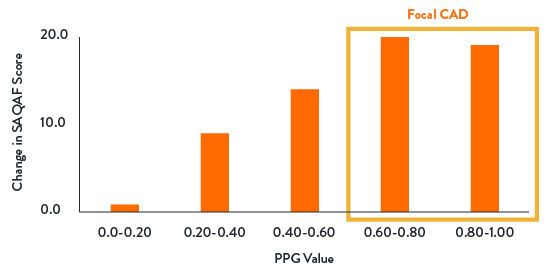
- PPG, a novel epicardial index, objectively quantifies focal epicardial disease to identify patients that are most likely to benefit from PCI32,33
- PPG is a continuous metric; values approaching 1.0 represent focal CAD, whereas values close to 0 diffuse CAD33
- EAPCI has recognized and endorsed the value of PPG in Pre-procedural PCI Planning to identify patterns of focal and diffuse disease37

Predict Patient Benefit
By measuring PPG, you can predict which patients are most likely to be angina-free post-PCI.32,35
- PPG demonstrated excellent predictive capacity for optimal revascularization
- PPG was significantly correlated with the change in post-PCI FFR32
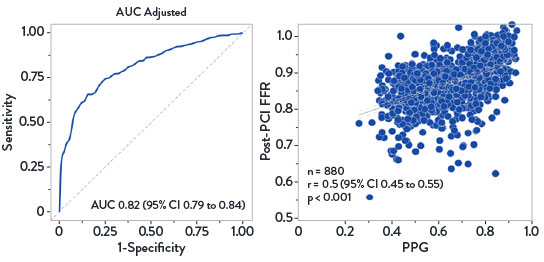
Predictive Capacity of PPG for FFR After PCI32
- Patients with high PPG (focal disease) reported greater improvement in angina and quality of life35
- PPG changed the revascularization decision in 1 out of 7 patients32
- Residual angina after PCI was ~2X more prevalent in patients with a low PPG (diffuse disease) than high PPG (focal)35
Change in Angina Frequency From Baseline to 1-Year Follow-Up36
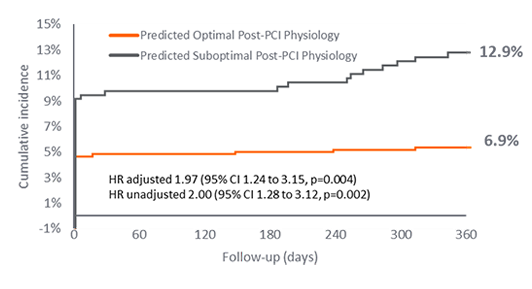
- One year outcomes from the PPG Global Study showed:
- PPG predicts suboptimal post-PCI physiology which is associated with higher rate of adverse events (TVF, MI, TVR).38
- PPG is the only independent predictor of angina improvement post-PCI within the study.38
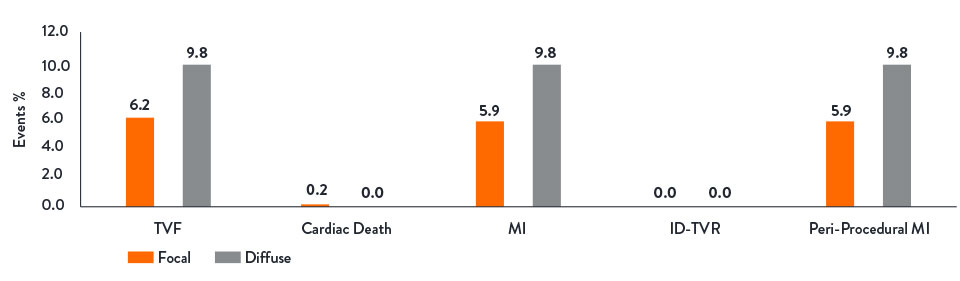
TVF38
Safe and Simple Workflow
The PPG Global Study demonstrated that PCI was safer to perform in patients with focal disease, resulting in lower rates of periprocedural MI.36
PPG integrates seamlessly into epicardial assessment workflow as a part of Abbott's Full Physiology solution.3,32,39
*As compared to all commercially available full physiology solutions outside of the U.S. as of Q1, 2026. Refer to IFUs for additional information. Full physiology refers to: Fractional Flow Reserve (FFR), Resting Full-cycle Ratio (RFR), Index of Microcirculatory Resistance (IMR), Coronary Flow Reserve (CFR) and Pullback Pressure Gradient (PPG).
References:
- Pijls, NH., et al. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996;334(26):1703-1708.
- Volcano Corp. Verrata‡ guidewire and PrimeWire Prestige‡ Plus guidewire IFUs, Opsens Inc. OptoWire‡ guidewire and OptoWire‡ II guidewire IFUs, ACIST Medical Systems. Navvus‡ Microcatheter IFU, Boston Scientific Corporation. Comet‡ guidewire IFU. Refer to IFUs for additional information.
- PressureWire™ X Guidewire Instructions for Use (IFU). Refer to IFU for additional information.
- Pijls, NH., et al. Fractional Flow Reserve Versus Angiography for Guiding Percutaneous Coronary Intervention in Patients with Multivessel Coronary Artery Disease. 2-Year Follow-Up of the FAME Study. JACC. 2010; 56(3): 177-184.
- Fearon, WF., et al. Fractional Flow Reserve-Guided PCI as Compared with Coronary Bypass Surgery. N Engl J Med, Nov 4, 2021.
- Boutaleb AM, et al. Fractional flow reserve and non-hyperemic indices: Essential tools for percutaneous coronary interventions. World J Clin Cases. 2023;11(10):2123-2139.
- Johnson NP, et al. Continuum of Vasodilator Stress From Rest to Contrast Medium to Adenosine Hyperemia for Fractional Flow Reserve Assessment. JACC Cardiovasc Interv. 2016;9(8):757-767l J Med, Nov 4, 2021.
- Corcoran, D., et al. Fractional flow reserve: a clinical perspective. Int J Cardiovasc Imaging. 2017;33(7):961‐974.
- Pijls, NH., et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol. 2010;56(3):177‐184.
- Smits, PC., et al. Fractional flow reserve–guided multivessel angioplasty in myocardial infarction. N Engl J Med. 2017; 376:1234-1244.
- Svanerud, J., et al. Validation of a novel non-hyperaemic index of coronary artery stenosis severity: the Resting Full-cycle Ratio (VALIDATE RFR) study. EuroIntervention. 2018;14:806-814.
- Lee, JM., et al. Physiological and clinical assessment of resting physiological indexes. Circulation. 2019;139:889-900.
- Jeremias, A., et al. Resting full-cycle ratio (RFR): a novel physiologic index compared to Fractional Flow Reserve (FFR) in assessing the hemodynamic severity of a coronary stenosis: ILUMIEN I + PREDICT. EuroPCR 2018.
- Ahn, JM., et al. IRIS FFR: prognostic performance of five resting pressure-derived indexes of coronary physiology. TCT 2018.
- Nam, CW., et al. Fractional flow reserve assessment of serial lesions. Radcliffe Cardiology. April 2014.
- Ali, Z., Invasive Assessment of Coronary Physiology Is Here to Stay! TCT 2019.
- Kumar, G., et al. RE-VALIDATE: REal world VALIDATion of the non-hyperemic InDex of coronary Artery sTEnosis severity: resting full-cycle ratio (RFR) – RE-VALIDATE RFR. CRT 2019.
- Lee, JM., et al. Clinical Outcome of Lesions with discordant results among different invasive physiologic indices. Circulation Journal 2019 83:2210-2221.
- Jeremias, A., et al. A Test in Context: FFR: Accuracy, Prognostic Implications, and Limitations. J AM Coll Cardiol. 2017; 69:2748-58.
- Veer, M., et al. Comparison of Different Diastolic Resting Indexes to iFR. J AM Coll Cardiol. 2017;70(25):3088-3096.
- Cook, C. Quantification of the Effect of Pressure Wire Drift on the Diagnostic Performance of FFR, iFR, & Pd/Pa. Circ Cardiovasc Interv. 2016;9(4):e002988.
- Mallidi, J., et al. Long-term outcomes following fractional flow reserve-guided treatment of angiographically ambiguous left main coronary artery disease: a meta-analysis of prospective cohort studies. Catheter Cardiovasc Interv. 2015;86(1):12-18.
- Johnson, NP., et al. Diastolic pressure ratio: new approach and validation vs the instantaneous wave-free ratio. Eur Heart J. 2019; 40(31):2585-2594
- Koo, BK., et al. Physiologic assessment of jailed side branch lesions using fractional flow reserve. J Am Coll Cardiol. 2005;46(4):633-637.
- Johnson, NP., et al. Prognostic value of fractional flow reserve: linking physiologic severity to clinical outcomes. J Am Coll Cardiol. 2014;64(16):1641-1654.
- Escaned, J., et al. Clinical outcomes of state-of-the-art percutaneous coronary revascularization in patients with de novo three vessel disease: 1-year results of the SYNTAX II study. Eur Heart J. 2017;38(42):3124-3134.
- DEFINE-FLAIR Trial Investigators. Comparison of major adverse cardiac events between instantaneous wave-free ratio and fractional flow reserve–guided strategy in patients with or without type 2 diabetes. JAMA Cardiol. 2019;4(9):857-864.
- Nijjer, SS., et al. Pre-angioplasty instantaneous wave-free ratio pullback provides virtual intervention and predicts hemodynamic outcome for serial lesions and diffuse coronary artery disease. JACC Cardiovasc Interv. 2014;7(12):1386-96.
- Jeremias, A., et al. Blinded physiological assessment of residual ischemia after successful angiographic percutaneous coronary intervention: the DEFINE PCI study. JACC Cardiovasc Interv. 2019;12(20):1991-2001.
- Sen, S., et al. Clinical events after deferral of LAD revascularization following physiological coronary assessment. J Am Coll Cardiol. 2019;73(4):444-453.
- Escaned, J., et al. Safety of the deferral of coronary revascularization on the basis of instantaneous wave-free ratio and fractional flow reserve measurements in stable coronary artery disease and acute coronary syndromes. JACC Cardiovasc Interv. 2018;11(15):1437-1449.
- Collet, C., et al. Influence of Pathophysiologic Patterns of Coronary Artery Disease on Immediate Percutaneous Coronary Intervention Outcomes. Circulation. 2024:150:586-597.
- Collet, C., et al. Measurement of Hyperemic Pullback Pressure Gradients to Characterize Patterns of Coronary Atherosclerosis. J Am Coll Cardiol. 2019;74(14):1772–1784.
- Mizukami, T., et al. Procedural Outcomes After Percutaneous Coronary Interventions in Focal and Diffuse Coronary Artery Disease. J Am Coll Cardiol Intv. 2022:11(23).
- Collet, C., et al. Differential Improvement in Angina and Health-Related Quality of Life After Percutaneous Coronary Interventions in Focal and Diffuse Coronary Artery Disease. J Am Coll Cardiol Intv. 2022;15:2506-2518.
- Collet, C., et al. Impact of Pullback Pressure Gradient (PPG) on Patient-Reported Outcomes in Patients with Coronary Artery Disease. Presented at TCT 2024.
- Escaned, J., et al. Applied coronary physiology for planning and guidance of percutaneous coronary interventions. A clinical consensus statement from European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the European Society of Cardiology. EuroIntervention 2023; 19:464-481.
- Ikeda, K., et al. Impact of Pullback Pressure Gradient on Clinical Outcomes after Percutaneous Coronary Interventions. Circ Cardiovasc Interv. 2025:e016022.
- CoroFlow‡ Cardiovascular System Instructions for Use (IFU). Refer to IFU for additional information.
- Data on file at Abbott.
MAT-2211667 v3.0