
Designed for Confidence
The Amplatzer Family of Duct Occluders offers an extensive line of devices and a simple treatment option for the closure of patent ductus arteriosus (PDA). Amplatzer™ Duct Occluders are designed to occlude PDAs of various shapes and sizes. With an easy-to-perform deployment procedure, the implanting physician can be confident in placing the device with precision.
Variety for PDA Occlusion
Amplatzer™ Duct Occluder
The Amplatzer™ Duct Occluder is designed to accommodate large PDAs with a single device — which may reduce the complexity of the procedure.

Amplatzer™ Duct Occluder II
The Amplatzer™ Duct Occluder II conforms to a variety of ducts while achieving complete closure from a pulmonary or aortic approach.1

Amplatzer Piccolo™ Occluder
The Amplatzer Piccolo™ Occluder, is designed to occlude small ducts in patients 700g and up, including neonates and infants.
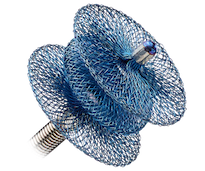
Optimal Design
Amplatzer Duct Occluders are flexible and conformable and can be securely positioned in the ductus for complete closure. They are constructed of Nitinol mesh and the Amplatzer Duct Occluder also has polyester material.
Get the Amplatzer Portfolio App
The Amplatzer Portfolio App helps physicians determine which Amplatzer Structural Interventions device to use by suggesting applicable devices based on respective Instructions for Use.

Download on the Apple App Store

Download on Google Play
Ordering Information
Amplatzer™ Duct Occluder
| Model/Reorder Number | Device Diameter at Descending Aorta (mm) | Device Diameter at Pulmonary Artery (mm) | Retention Skirt Diameter (mm) | Device Length (mm) |
|---|---|---|---|---|
| 9-PDA-003 | 5 | 4 | 9 | 5 |
| 9-PDA-004 | 6 | 4 | 10 | 7 |
| 9-PDA-005 | 8 | 6 | 12 | 7 |
| 9-PDA-006 | 10 | 8 | 16 | 8 |
| 9-PDA-007 | 12 | 10 | 18 | 8 |
Amplatzer™ Duct Occluder II
| Model/Reorder Number | Waist Diameter (mm) | Device Length (mm) | Disc Diameter (mm) |
|---|---|---|---|
| 9-PDA2-03-04 | 3 | 4.25 | 9 |
| 9-PDA2-03-06 | 3 | 6.25 | 9 |
| 9-PDA2-04-04 | 4 | 4.25 | 10 |
| 9-PDA2-04-06 | 4 | 6.25 | 10 |
| 9-PDA2-05-04 | 5 | 4.25 | 11 |
| 9-PDA2-05-06 | 5 | 6.25 | 11 |
| 9-PDA2-06-04 | 6 | 4.25 | 12 |
| 9-PDA2-06-06 | 6 | 6.25 | 12 |
Amplatzer Piccolo™ Occluder
| Model/Reorder Number | Waist Diameter (mm) [A] | Length betweek discs (mm) [B] | Disc Diameter (mm) [C] | Recommended Sheath Size |
|---|---|---|---|---|
| 9-PDAP-03-02-L | 3 | 2 | 4.00 | 4 F; 90° Curve |
| 9-PDAP-03-04-L | 3 | 4 | 4.00 | 4 F; 90° Curve |
| 9-PDAP-03-06-L | 3 | 6 | 4.00 | 4 F; 90° Curve |
| 9-PDAP-04-02-L | 4 | 2 | 5.25 | 4 F; 90° Curve |
| 9-PDAP-04-04-L | 4 | 4 | 5.25 | 4 F; 90° Curve |
| 9-PDAP-04-06-L | 4 | 6 | 5.25 | 4 F; 90° Curve |
| 9-PDAP-05-02-L | 5 | 2 | 6.50 | 4 F; 90° Curve |
| 9-PDAP-05-04-L | 5 | 4 | 6.50 | 4 F; 90° Curve |
| 9-PDAP-05-06-L | 5 | 6 | 6.50 | 4 F; 90° Curve |
References
- Saliba Z, El-Rassi I, Abi-Warde M T, et al. The Amplatzer Duct Occluder II: a new device for percutaneous ductus arteriosus closure. Journal of Interventional Cardiology. 2009;22(6):496-502.
Rx Only
Important Safety Information
AMPLATZER™ DUCT OCCLUDER II
Indications for Use
The AmplatzerTM Duct Occluder II is a percutaneous transcatheter occlusion device intended for the non-surgical closure of patent ductus arteriosus.
Contraindications
The AmplatzerTM Duct Occluder II is contraindicated for the following: Patients weighing less than 6 kg; Patients less than 6 months of age; Patients with a window-type patent ductus arteriosus (ie, length less than 3mm); Patients with an active infection; Patients with thrombus at the intended site of implant; Patients with pulmonary hypertension with pulmonary vascular resistance of greater than 8 Wood units or Rp/Rs of greater than 0.4; Patients with patent ductus arteriosus greater than 12 mm in length by angiography; Patients with patent ductus arteriosus greater than 5.5 mm in diameter by angiography.
Potential Adverse Events
Potential adverse events that may occur during or after a procedure using this device may include, but are not limited to: Air embolus; Allergic dye reaction; Allergic drug reaction; Anesthesia reactions; Apnea; Arrhythmia; Bacterial endocarditis; Bleeding; Cardiac perforation; Cardiac tamponade; Chest pain; Device embolization; Device erosion; Death; Fever; Headache/migraine; Hypertension; Hypotension; Myocardial infarction; Palpitations; Pericardial effusion; Pericarditis; Peripheral embolism; Pleural effusion; Pulmonary embolism; Reintervention for device removal; Stroke; Transient ischemic attack; Thrombus; Valvular regurgitation; Vascular access site injury; Vessel perforation.
Rx Only
Important Safety Information
AMPLATZER PICCOLO™ OCCLUDER
Indication of Use
The Amplatzer Piccolo™ Occluder is a percutaneous, transcatheter occlusion device intended for the nonsurgical closure of a patent ductus arteriosus (PDA).
Contraindications
Weight < 700 grams at time of the procedure; Age < 3 days at time of procedure; Coarctation of the aorta; Left pulmonary artery stenosis; Cardiac output that is dependent on right to left shunt through the PDA due to pulmonary hypertension; Intracardiac thrombus that may interfere with the implant procedure; Active infection requiring treatment at the time of implant; Patients with a PDA length smaller than 3 mm; Patients with a PDA diameter that is greater than 4 mm at the narrowest portion.
Potential adverse events
Potential adverse events that may occur during or after a procedure using this device may include, but are not limited to: Air embolus, Allergic reaction, Anemia, Anesthesia reactions, Apnea, Arrhythmia, Bleeding, Cardiac perforation, Cardiac tamponade, Chest pain, Device embolization, Device erosion, Death, Endocarditis, Fever, Headache/migraine, Hemolysis, Hematoma, Hypertension, Hypotension, Infection, Myocardial infarction, Palpitations, Partial obstruction of aorta, Partial obstruction of pulmonary artery, Pericardial effusion, Pericarditis, Peripheral embolism, Pleural effusion, Pulmonary embolism, Re-intervention for device removal, Respiratory distress, Stroke, Thrombus, Transient ischemic attack, Valvular regurgitation, Vascular access site injury, Vascular occlusion, Vessel perforation.
MAT-2006762 v2.0