- RFR scans through diastole and systole for the largest drop in pressure in the entire cardiac cycle.
- RFR has been studied in over 3,500 lesions and 2,500 patients1-5 and RFR has shown diagnostic equivalence to iFR.6

"The major advantage of RFR over iFR‡ is that RFR does not require identification of a specific landmark or selection of a specific time point during diastole. By calculating the minimum Pd/Pa over the entire cardiac cycle, RFR calculates the maximum pressure gradient across the stenosis during resting status." 5
– Lee, et al. Circulation 2019
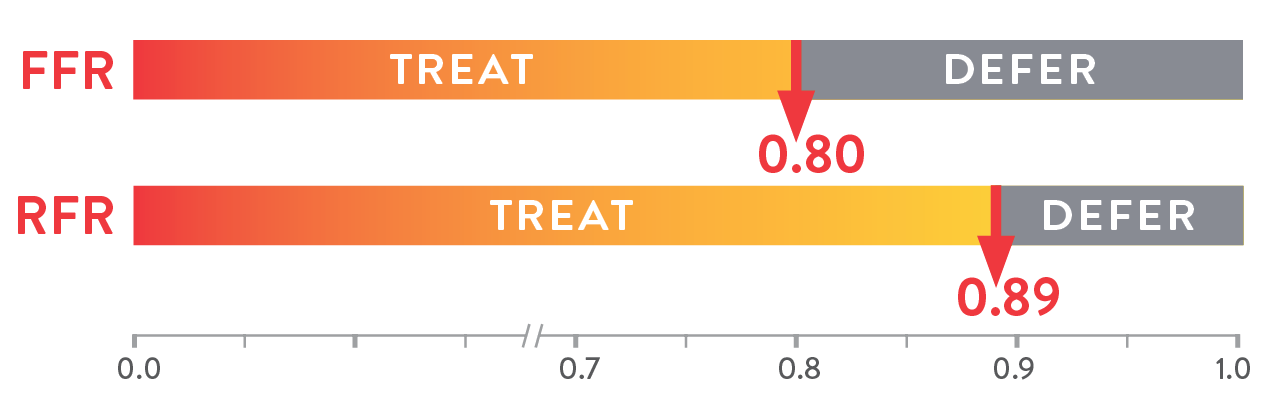
The cutoff value of RFR is 0.89:1-3
All resting pressure-derived indices closely correlate with one another, revealing the same discriminatory ability to guide intervention.5 The large IRIS-FFR retrospective study (1,506 patients, 1,833 lesions) examined deferred lesion failure among 5 resting indices—resting Pd/Pa, iFR‡, RFR, dPR‡, and DFR‡—and concluded that all resting indices had similar outcomes in deferred lesions.1

Here are the cutoff values for the various non-hyperemic pressure ratios.8

Coronary angiography is not accurate in guiding the functional significance of stenosis in 34% of cases, compared to FFR.9

FFR-guided percutaneous coronary intervention (PCI) leads to a 35% risk reduction in death and myocardial infarction (MI), compared to relying only on angiography.10

Complete revascularization with PressureWire™ X Guidewire led to a 62% relative risk reduction in major adverse cardiac and cerebrovascular events (MACCE) at 1 year.11 The COMPARE-ACUTE trial also revealed that untreated “FFR-positive” non-infarct-related artery lesions are associated with a 31% incidence of MACCE at 1 year.11


Previous Sensor Jacket with single "window"

Updated Sensor Jacket with multiple larger "windows"
Drift is a phenomenon that affects the accuracy of most pressure measurement devices.13 Accuracy is particularly critical for resting ratios, as clinical decisions from resting ratios are more impacted by drift than FFR.14,15
Compared to the hyperemic state, smaller separation between Pd and Pa at rest means even relatively small amounts of drift can lead to stenosis misclassification compared to FFR (Figure below). Therefore, it is critical to detect even the slightest difference of pressure.


Coronary angiography, the primary diagnostic test for angina, cannot assess the microcirculation, which is largely responsible for the regulation and distribution of blood flow to the myocardium.16 Patients with persistent angina—but non-obstructive coronary artery disease (NOCAD) on angiography—often remains undiagnosed.13
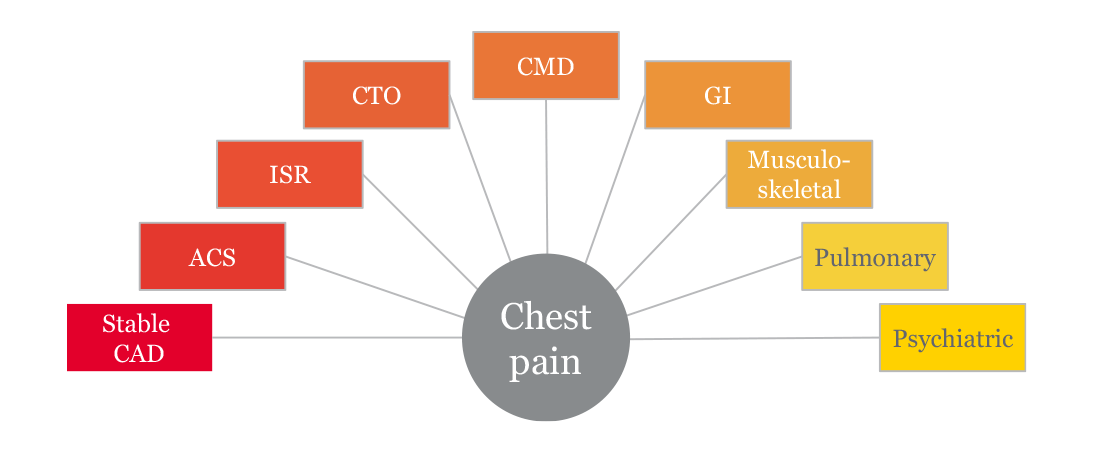
Ischemic heart disease continues to be the leading cause of death globally.18 Yet chest pain—while often ischemic in nature—could have many etiologies (illustration below).
To improve outcomes in these patients at high risk for major adverse cardiac events (MACE), proper diagnosis of CMD and management is essential16,17 and depends on accurately identifying and treating the underlying cause of angina.
The PressureWire™ X Guidewire and Coroventis‡ CoroFlow‡ Cardiovascular System can measure both IMR and CFR - allowing for a CMD diagnosis.19
Microvascular angina and vasospastic angina are the two most common causes of INOCA, and both types of angina can be identified with diagnostic testing. The randomised CorMicA trial provides a diagnostic and treatment approach.20
The trial protocol assessed patients to determine20:
The CorMicA results indicate a role for a more thorough investigation of coronary dysfunction among patients with INOCA, as well as an opportunity to better tailor patient treatment.20
‡ Indicates a third-party trademark, which is property of its respective owner.
References:
1. Ahn JM, et al. IRIS FFR: prognostic performance of five resting pressure-derived indexes of coronary physiology. TCT 2018.
2. Jeremias A, et al. Resting full-cycle ratio (RFR): a novel physiologic index compared to Fractional Flow Reserve (FFR) in assessing the hemodynamic severity of a coronary stenosis: ILUMIEN I + PREDICT. EuroPCR 2018.
3. Svanerud J, et al. Validation of a novel non-hyperaemic index of coronary artery stenosis severity: the Resting Full-cycle Ratio (VALIDATE RFR) study. EuroIntervention. 2018;14:806-814.
4. Kumar et al. Re-VALIDATE RFR. CRT 2019.
5. Lee J-M, et al. Physiological and clinical assessment of resting physiological indexes. Circulation. 2019;139.
6. Volcano Corp. Verrata guidewire and PrimeWire Prestige Plus guidewire IFUs, Opsens Inc. OptoWire guidewire and OptoWire II guidewire IFUS, ACIST Medical Systems. Navvus Microcatheter IFU, Boston Scientific Corporation. Comet‡ guidewire IFU, PressureWire™ X guidewire IFU.
7. Tonino PA, et al. Angiographics versus functional severity of coronary artery stenoses in the FAME study: Fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol 2010; 55:2816-21.
8. Ali ZA. Invasive assessment of coronary physiology is here to stay. TCT 2019.
9. Corcoran D, Hennigan B, Berry C. Fractional flow reserve: a clinical perspective. Int J Cardiovasc Imaging. 2017;33(7):961‐974. doi:10.1007/s10554-017-1159-2
10. Pijls NH, Fearon WF, Tonino PA, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol. 2010;56(3):177‐184. doi:10.1016/j.jacc.2010.04.012
11. Smits PC, Abdel-Wahab M, Neumann FJ, et al. Fractional flow reserve–guided multivessel angioplasty in myocardial infarction. N Engl J Med. 2017; 376:1234-1244. doi:10.1056/NEJMoa1701067.
12. Abbott data on file. Report 90328885.
13. Jeremias, A., et al. A Test in Context: FFR: Accuracy, Prognostic Implications, and Limitations. JACC 2017; 69:2748-58.
14. Van’t Veer, M, et al. JACC. Comparison of Different Diastolic Resting Indexes to iFR. 70 (25), 2017.
15. Cook, C. CCI. Quantification of the Effect of Pressure Wire Drift on the Diagnostic Performance of FFR, iFR, & Pd/Pa.
16. Taqueti VR, Di Carli MF. Coronary microvascular disease pathogenic mechanisms and therapeutic options: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72:2625–2641. doi:10.1016/j.jacc.2018.09.042.
17. Jespersen L, Hvelplund A, Abildstrøm SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734-744. doi:10.1093/eurheartj/ehr331.
18. Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1459-544.
19. PressureWire™ X guidewire IFU. Coroventis CoroFlow Cardiovascular System IFU.
20. Ford TJ, Stanley B, Sidik N, et al. 1-year outcomes of angina management guided by invasive coronary function testing (CorMicA). J Am Coll Cardiol Intv. 2020;13:33-45.
Date of preparation: May 2021. SFM_ABO1755.
MAT-2105207 v1.0
Please be aware that the website you have requested is intended for the residents of a particular country or countries, as noted on that site. As a result, the site may contain information on pharmaceuticals, medical devices and other products or uses of those products that are not approved in other countries or regions
MAT-2105201 v1.0