
To discover the root cause of persistent angina, patients may need an accurate diagnosis for Coronary Microvascular Dysfunction (CMD) that requires more than the angiogram alone.1 Comprehensive physiology testing of both the epicardial arteries and microcirculation can help provide a clear diagnosis to guide treatment and improve patient outcomes.2
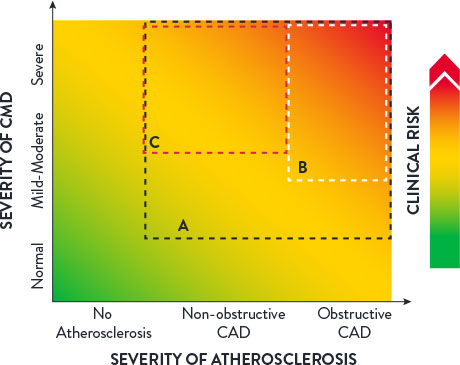
The microcirculation carries far more myocardial blood volume compared to the epicardial arteries. CMD can be defined as impaired blood flow to the microcirculation, which is largely responsible for the regulation and distribution of blood flow to the myocardium.1
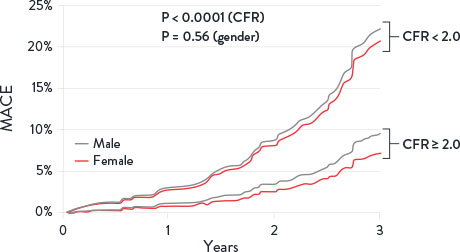
Patients with INOCA can be diagnosed for CMD by measuring Index of Microcirculatory Resistance (IMR) and Coronary Flow Reserve (CFR).3 Patients with abnormal CFR have an increase in major adverse cardiac events (MACE) including:
Additionally, these patients have an increase in diastolic dysfunction and cardiac death.4
A clear, accurate CMD diagnosis can help reduce healthcare resource consumption.5
40-60% of all elective patients undergoing angiography suffer from INOCA. Up to half of this patient population might have angina due to CMD.11,12
Understanding the symptoms may help you determine if your patient could benefit from comprehensive physiology testing. Patients suffering from CMD may include:8
Other symptoms may include chest pain, shortness of breath, and more.

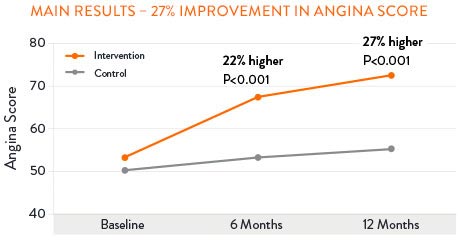
The CorMicA (Coronary Microvascular Angina) study revealed that patients may benefit when CMD is accurately diagnosed and appropriately treated. 27% of patients saw improvement in angina severity at 1 year with optimized medical therapy.17
Sustained Angina Improvement with CMD Treatment17,†
PressureWire™ X Guidewire with the CoroFlow‡ Cardiovascular System is the only* solution for the catherization laboratory able to assess both the epicardial arteries and the microvasculature that can give patients the accurate diagnosis that they deserve.17,18,19
Connect with your partnering referring physician to discuss how your access to the PressureWire™ X Guidewire and CoroFlow‡ Cardiovascular System can benefit their patients with angina and no angiographic abnormalities.
Learn more about PressureWire™ X Guidewire and CoroFlow‡ Cardiovascular System.

*With Index of Microcirculatory Resistance (IMR), Coronary Flow Reserve (CFR), Fractional Flow Reserve (FFR) and Resting Full-Cycle Ratio (RFR).
†According to the Seattle Angina Questionaire score.
MAT-2206706 v2.0
You are about to enter an Abbott country- or region-specific website.
Please be aware that the website you have requested is intended for the residents of a particular country or countries, as noted on that site. As a result, the site may contain information on pharmaceuticals, medical devices and other products or uses of those products that are not approved in other countries or regions
Do you wish to continue and enter this website?
MAT-2305078 v1.0