
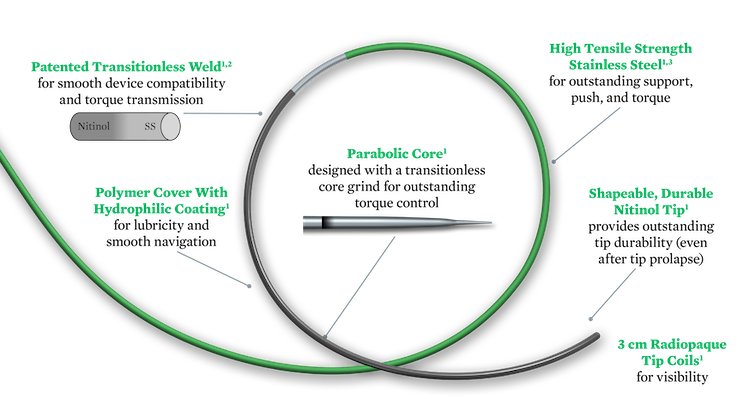
Hybrid workhorse guide wires combine the key advantages of nitinol wires and stainless steel wires.1

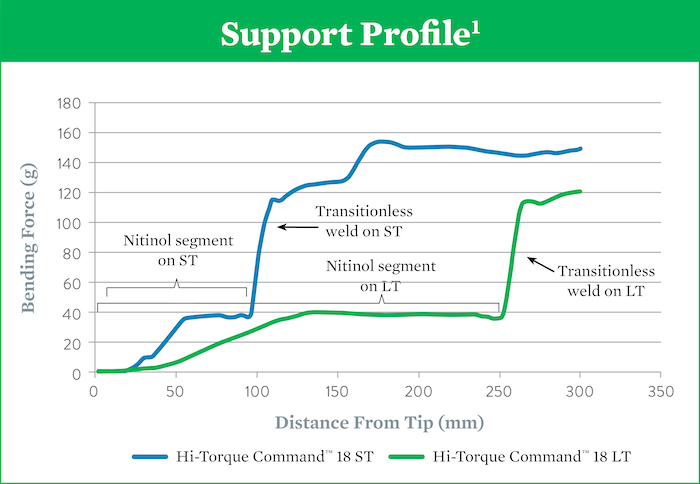
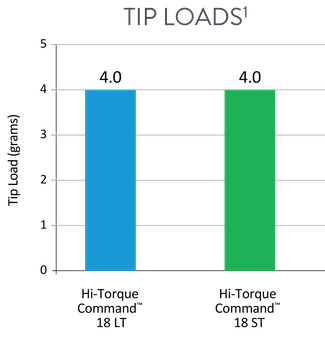
Crossing wire, with 10 cm nitinol at distal end, provides high support and a flexible tip (4g) for crossing lesions or prolapsing in a tight loop.1
Navigation wire, with 25 cm nitinol at distal end, provides flexible support and a soft tip (4g) to effectively track through tortuous peripheral vessels.1
| Product | Part Number | Diameter | Length | Nitinol Length | Tip Load | Tip Shape |
|---|---|---|---|---|---|---|
| Hi-Torque Command™ 18 ST | 1013730 | 0.018 in | 210 cm | 10 cm | 4 g | Straight |
| Hi-Torque Command™ 18 ST | 1013731 | 0.018 in | 300 cm | 10 cm | 4 g | Straight |
| Hi-Torque Command™ 18 LT | 1013752 | 0.018 in | 210 cm | 25 cm | 4 g | Straight |
| Hi-Torque Command™ 18 LT | 1013753 | 0.018 in | 300 cm | 25 cm | 4 g | Straight |
Hi-Torque Command™ 18 guide wire is packaged with a torque device and guide wire introducer that can be used for tip shaping.1
References:
MAT-2006301 v2.0

INDICATIONS FOR USE
This Hi-Torque™ Guide Wire is intended to facilitate the placement of balloon dilatation catheters during percutaneous transluminal angioplasty (PTA), in arteries such as the femoral, popliteal and infra-popliteal arteries.This guide wire may also be used with compatible stent devices during therapeutic procedures.
The guide wire may also be used to reach and cross a target lesion, provide a pathway within the vessel structure, facilitate the substitution of one diagnostic or interventional device for another, and to distinguish the vasculature.
CONTRAINDICATIONS
Not intended for use in the coronary or cerebral vasculature.
WARNINGS
This device is not designed for use with artherectomy devices.
This device is designed and intended for ONE-TIME USE ONLY. Do not resterilize and / or reuse.
Carefully observe the instructions under “Do Not” and “Do” below. Failure to do so may result in vessel trauma, guide wire damage, guide wire tip separation, or stent damage. If resistance is observed at any time, determine the cause under fluoroscopy and take remedial action as needed. Use the most suitable guide wire for the lesion being treated.
Do Not:
PRECAUTIONS
Guide wires are delicate instruments and should be handled carefully. Prior to use and when possible during the procedure, inspect the guide wire carefully for bends, kinks, or other damage. Do not use damaged guide wires. Using a damaged guide wire may result in vessel damage and / or inaccurate torque response.
Confirm the compatibility of the guide wire diameter with the interventional device before actual use.
Free movement of the guide wire within the interventional device is an important feature of a steerable guide wire system, because it gives the user valuable tactile information. Test the system for any resistance prior to use. Adjust or replace the hemostatic valve with an adjustable valve if it is found to inhibit guide wire movement.
Avoid abrasion of the hydrophilic coating.
Do not withdraw or manipulate the hydrophilic-coated wire through a metal cannula or sharp-edged object.
ADVERSE EVENTS (AEs)
Potential Adverse Events associated with use of this device may include the following but are not limited to:
MAT-2111768 v2.0
STAY CONNECTED